Vous aimerez peut-être aussi
- Noise Induced Hearing Loss (Nihl) : Bsuir Scientific Conference APRIL 2015Document21 pagesNoise Induced Hearing Loss (Nihl) : Bsuir Scientific Conference APRIL 2015muhammadPas encore d'évaluation
- Procesamiento de Información EstadísticaDocument8 pagesProcesamiento de Información EstadísticaDanna Evioleth Torres RamosPas encore d'évaluation
- Isbn 9789526051727Document82 pagesIsbn 9789526051727jorgeortizramos1936Pas encore d'évaluation
- Occupational and Environmental Health: Prepared by Ms Yasmeen Bibi MR Asif ShahDocument67 pagesOccupational and Environmental Health: Prepared by Ms Yasmeen Bibi MR Asif ShahAamirPas encore d'évaluation
- New Developments of PetDocument59 pagesNew Developments of Petmm_555_ssPas encore d'évaluation
- Comparing Statistics Class Exam Scores and Drug Trial ResultsDocument2 pagesComparing Statistics Class Exam Scores and Drug Trial ResultssivaPas encore d'évaluation
- Objectives Appraisal Jan-April 2020Document15 pagesObjectives Appraisal Jan-April 2020mbeng bessonganyiPas encore d'évaluation
- HTML To PDFDocument1 pageHTML To PDFYesenia GaleotePas encore d'évaluation
- HDFC Developed World Indexes Fund of FundsDocument13 pagesHDFC Developed World Indexes Fund of FundsArmstrong CapitalPas encore d'évaluation
- Lecture 6 - Industrial WastewaterDocument51 pagesLecture 6 - Industrial Wastewaterjefferson atienzaPas encore d'évaluation
- Dosh OshaDocument33 pagesDosh OshaMasri Bin TaminPas encore d'évaluation
- Theory of National Income DeterminationDocument50 pagesTheory of National Income DeterminationKunal KunduPas encore d'évaluation
- Poucv: Intermediary Code Intermediary Name ContactDocument2 pagesPoucv: Intermediary Code Intermediary Name ContactMahendar ErramPas encore d'évaluation
- Digital Implant Planning and Guided Implant Surgery Workflow and ReliabilityDocument8 pagesDigital Implant Planning and Guided Implant Surgery Workflow and ReliabilityDenisa CorneaPas encore d'évaluation
- Smart Champ Insurance Brochure 2017Document12 pagesSmart Champ Insurance Brochure 2017RahulPas encore d'évaluation
- The Business CycleDocument24 pagesThe Business CycleAman Raj 'VII'GPas encore d'évaluation
- PAES 307 Agricultural Helical Gears SpecsDocument31 pagesPAES 307 Agricultural Helical Gears SpecsJemina Jean Dorado SensanoPas encore d'évaluation
- Fan 7371Document1 pageFan 7371Leonardo GomesPas encore d'évaluation
- Noise Report 2021Document32 pagesNoise Report 2021JESUS BASILIO ANTONIOPas encore d'évaluation
- Navy FY 2011 Budget for Research, Development, Test and EvaluationDocument1 330 pagesNavy FY 2011 Budget for Research, Development, Test and EvaluationkarakogluPas encore d'évaluation
- PPM Visualization ToolkitDocument31 pagesPPM Visualization ToolkitTaha ShahzadPas encore d'évaluation
- Sla Folder Na - enDocument4 pagesSla Folder Na - enlukito lukitoPas encore d'évaluation
- Electrical Safety DocumentDocument12 pagesElectrical Safety DocumentRajeev SharmaPas encore d'évaluation
- Cellular Effects Related To The Clinical Uses of Laser in OrthodonticsDocument5 pagesCellular Effects Related To The Clinical Uses of Laser in Orthodonticsmonwarul azizPas encore d'évaluation
- Screenshot 2024-03-05 at 4.04.17 AMDocument41 pagesScreenshot 2024-03-05 at 4.04.17 AMmalakbinthaniPas encore d'évaluation
- SafetyDocument25 pagesSafetyAlvinPas encore d'évaluation
- OR Connection Magazine - Volume 5 Issue 1Document96 pagesOR Connection Magazine - Volume 5 Issue 1medlineUPas encore d'évaluation
- Global Strategy For Asthma Management and Prevention: OR DistributeDocument211 pagesGlobal Strategy For Asthma Management and Prevention: OR DistributeHenny Rahmawati100% (1)
- GINA 2020 Full Report - Final - Wms PDFDocument211 pagesGINA 2020 Full Report - Final - Wms PDFAngelica IpardjoPas encore d'évaluation
- Low Btu GasDocument15 pagesLow Btu Gaszubair1950Pas encore d'évaluation
- Sustainable Development Report 2011 2012Document28 pagesSustainable Development Report 2011 2012Dario Vivanco HuaytaraPas encore d'évaluation
- 229 Priyankar Biswas Wage DeterminationDocument9 pages229 Priyankar Biswas Wage DeterminationArik Das100% (1)
- Intelligent and Green BuildingsDocument35 pagesIntelligent and Green Buildingsmagda badrPas encore d'évaluation
- 1Document13 pages1RoseRose7Pas encore d'évaluation
- Zirconia in Dentistry Part 2. Evidence-BDocument33 pagesZirconia in Dentistry Part 2. Evidence-Bt723849Pas encore d'évaluation
- Ssa Heads MeetingDocument4 pagesSsa Heads MeetingYssreddy SivasankarareddyPas encore d'évaluation
- Presentation20ED20Day20Honeck 1Document7 pagesPresentation20ED20Day20Honeck 1Mariell LunaPas encore d'évaluation
- Channel Marketing Budget TemplateDocument4 pagesChannel Marketing Budget TemplateianachieviciPas encore d'évaluation
- GDP & Output Change: Potential Impact On Key AreasDocument2 pagesGDP & Output Change: Potential Impact On Key AreasDEEPAK BHASMEPas encore d'évaluation
- VIR - Reform in TelecommunicationsDocument10 pagesVIR - Reform in TelecommunicationsNgu HoangPas encore d'évaluation
- Unintended Changes To The Occlusion Following The Provision of Night GuardsDocument8 pagesUnintended Changes To The Occlusion Following The Provision of Night Guardsjorge230956Pas encore d'évaluation
- 10 1 1 457 7733 PDFDocument12 pages10 1 1 457 7733 PDFfranobeljo27Pas encore d'évaluation
- Desktop - 1Document1 pageDesktop - 1Youtube PremiumPas encore d'évaluation
- PrimeroDocument23 pagesPrimeroCarlos Andrés González RodríguezPas encore d'évaluation
- Adjustable NebuliserDocument1 pageAdjustable NebuliserHaiat AlsuwaidiPas encore d'évaluation
- Pruksa, V1N1A5Document6 pagesPruksa, V1N1A5supakit456453Pas encore d'évaluation
- But Is India Doing Enough To Meet Its Present and Future Needs?Document48 pagesBut Is India Doing Enough To Meet Its Present and Future Needs?Vlad BrătfăleanPas encore d'évaluation
- Bandhan Focused Equity FundDocument10 pagesBandhan Focused Equity FundArmstrong CapitalPas encore d'évaluation
- Regional Imbalances: Chapter - 7Document31 pagesRegional Imbalances: Chapter - 7roy_esha86Pas encore d'évaluation
- 17nov pp2Document20 pages17nov pp2Zhang YuchiPas encore d'évaluation
- TR Implementation On The Medical Assistance To Walk in Clients03072022125917Document18 pagesTR Implementation On The Medical Assistance To Walk in Clients03072022125917azereth bartonPas encore d'évaluation
- Coronectomy of an impacted deciduous molarDocument2 pagesCoronectomy of an impacted deciduous molarRosel SalazarPas encore d'évaluation
- Erso Country Overview 2023 Germany - 0Document25 pagesErso Country Overview 2023 Germany - 0bninvestbaliPas encore d'évaluation
- Statistics Analyses InsightsDocument15 pagesStatistics Analyses Insightssam aliPas encore d'évaluation
- 라.+발표자료Document58 pages라.+발표자료dangvu16022002Pas encore d'évaluation
- WN REA Reen OU R: Team-Y.O.G.ADocument17 pagesWN REA Reen OU R: Team-Y.O.G.AYoga Plant DecorPas encore d'évaluation
- Fossil Fuels' Energy and Their Environmental Impact: April 12, 2005Document51 pagesFossil Fuels' Energy and Their Environmental Impact: April 12, 2005DaisyPas encore d'évaluation
- 4gre Y4108Document1 page4gre Y4108kuraimundPas encore d'évaluation
- 4 Exposure Criteria, Occupational Exposure LevelsDocument24 pages4 Exposure Criteria, Occupational Exposure LevelsTunjungsPas encore d'évaluation
- Banking Automation: Data Processing Systems and Associated EquipmentD'EverandBanking Automation: Data Processing Systems and Associated EquipmentPas encore d'évaluation
- Cirugi A Espan Ola: Treatment of Thyroid Follicular CarcinomaDocument8 pagesCirugi A Espan Ola: Treatment of Thyroid Follicular CarcinomamawarmelatiPas encore d'évaluation
- Zometa Epar Product Information enDocument112 pagesZometa Epar Product Information enmawarmelatiPas encore d'évaluation
- Abalaka Et AlDocument5 pagesAbalaka Et AlmawarmelatiPas encore d'évaluation
- Antimicrobial Activity of Ber FruitDocument4 pagesAntimicrobial Activity of Ber FruitmawarmelatiPas encore d'évaluation
- Short CommunicationDocument7 pagesShort CommunicationmawarmelatiPas encore d'évaluation
- Jawt 12 I 2 P 61Document3 pagesJawt 12 I 2 P 61mawarmelatiPas encore d'évaluation
- Case Report Dentigerous Cyst in Maxillary Sinus: A Rare OccurrenceDocument5 pagesCase Report Dentigerous Cyst in Maxillary Sinus: A Rare OccurrencemawarmelatiPas encore d'évaluation
- AutisminreviewDocument7 pagesAutisminreviewmawarmelatiPas encore d'évaluation
- 1 SMDocument8 pages1 SMmawarmelatiPas encore d'évaluation
- Tonsillitis: Christos C. Georgalas, Neil S. Tolley, and Antony NarulaDocument14 pagesTonsillitis: Christos C. Georgalas, Neil S. Tolley, and Antony NarulaArthuria PendragonPas encore d'évaluation
- Z-Plasty Method in Tracheostomal Stenosis Repair: A Case ReportDocument2 pagesZ-Plasty Method in Tracheostomal Stenosis Repair: A Case ReportmawarmelatiPas encore d'évaluation
- Asian Journal of Oral and Maxillofacial Surgery: Invasive Carcinoma Ex Pleomorphic Adenoma of Submandibular Gland: A CaseDocument3 pagesAsian Journal of Oral and Maxillofacial Surgery: Invasive Carcinoma Ex Pleomorphic Adenoma of Submandibular Gland: A CasemawarmelatiPas encore d'évaluation
- Tonsillitis: Christos C. Georgalas, Neil S. Tolley, and Antony NarulaDocument14 pagesTonsillitis: Christos C. Georgalas, Neil S. Tolley, and Antony NarulaArthuria PendragonPas encore d'évaluation
- 113 Full PDFDocument5 pages113 Full PDFDeniPas encore d'évaluation
- SquamousDocument10 pagesSquamousElaine TalusanPas encore d'évaluation
- 0 Clinical Original Contribution: J. FRCR, N. JDocument4 pages0 Clinical Original Contribution: J. FRCR, N. JmawarmelatiPas encore d'évaluation
- Alshagroud2017 Article MetastasizingPleomorphicAdenomDocument7 pagesAlshagroud2017 Article MetastasizingPleomorphicAdenommawarmelatiPas encore d'évaluation
- Surgical Approaches To Submandibular GlandDocument7 pagesSurgical Approaches To Submandibular GlandNarla SusheelPas encore d'évaluation
- Pleomorphic Multicentric Adenoma Submandibular GlandDocument3 pagesPleomorphic Multicentric Adenoma Submandibular GlandmawarmelatiPas encore d'évaluation
- OkeDocument7 pagesOkemawarmelatiPas encore d'évaluation
- Submandibular Gland Excision OutcomesDocument4 pagesSubmandibular Gland Excision OutcomesmawarmelatiPas encore d'évaluation
- Case Report Dentigerous Cyst in Maxillary Sinus: A Rare OccurrenceDocument5 pagesCase Report Dentigerous Cyst in Maxillary Sinus: A Rare OccurrencemawarmelatiPas encore d'évaluation
- Z-Plasty Method in Tracheostomal Stenosis Repair: A Case ReportDocument2 pagesZ-Plasty Method in Tracheostomal Stenosis Repair: A Case ReportmawarmelatiPas encore d'évaluation
- Tingkat Pengetahuan Dan Kesadaran Pelajar Terhadap Kanker Rongga MulutDocument11 pagesTingkat Pengetahuan Dan Kesadaran Pelajar Terhadap Kanker Rongga MulutAnonymous f2FL9OplfwPas encore d'évaluation
- Squamous Cell Carcinoma of Tympanomastoid Region - A Rare and Often Misdiagnosed EntityDocument4 pagesSquamous Cell Carcinoma of Tympanomastoid Region - A Rare and Often Misdiagnosed EntitymawarmelatiPas encore d'évaluation
- Description of Odontogenic Infection Cases at The Oral Surgery Polyclinic of Hasan Sadikin Hospital Bandung, IndonesiaDocument6 pagesDescription of Odontogenic Infection Cases at The Oral Surgery Polyclinic of Hasan Sadikin Hospital Bandung, IndonesiamawarmelatiPas encore d'évaluation
- Isd 41 189Document5 pagesIsd 41 189mawarmelatiPas encore d'évaluation
- Isd 41 189Document5 pagesIsd 41 189mawarmelatiPas encore d'évaluation
- FistelDocument3 pagesFistelmawarmelatiPas encore d'évaluation
- SaidatulAqilah 5 1 A3Document10 pagesSaidatulAqilah 5 1 A3mawarmelatiPas encore d'évaluation
- The Duchess DealDocument269 pagesThe Duchess DealDharshena100% (11)
- 8086 Instruction Set and Assembly Language ProgramDocument13 pages8086 Instruction Set and Assembly Language Programwaheed azizPas encore d'évaluation
- RADIALL - RP66393 Plug With Backshell CapDocument1 pageRADIALL - RP66393 Plug With Backshell CapIlaiarajaPas encore d'évaluation
- Strategies in Teaching Social Studies Inductive and Deductive Andragogy vs. PedagogyDocument31 pagesStrategies in Teaching Social Studies Inductive and Deductive Andragogy vs. PedagogyArvie VillegasPas encore d'évaluation
- Pending 1667646640 ForeclosureSimulationDocument2 pagesPending 1667646640 ForeclosureSimulationpramod roy0% (1)
- Indian Railways Service of Engineers: A Glorious ServiceDocument5 pagesIndian Railways Service of Engineers: A Glorious ServiceHabib Ur RahmanPas encore d'évaluation
- Design Calculation: Season 2 - Mechanical and Chemical Anchor CalculationDocument23 pagesDesign Calculation: Season 2 - Mechanical and Chemical Anchor CalculationNaveenPas encore d'évaluation
- q2 w6 Asteroids Comets MeteorsDocument61 pagesq2 w6 Asteroids Comets MeteorsxenarealePas encore d'évaluation
- At.3212 - Determining The Extent of TestingDocument12 pagesAt.3212 - Determining The Extent of TestingDenny June CraususPas encore d'évaluation
- CarpentaryDocument10 pagesCarpentaryvikrantPas encore d'évaluation
- Interest SwapsDocument6 pagesInterest SwapsamiPas encore d'évaluation
- Metal Bollards Installation Risk AssessmentDocument7 pagesMetal Bollards Installation Risk AssessmentEldhose VarghesePas encore d'évaluation
- 9.36 Project Summary FormDocument2 pages9.36 Project Summary FormTu Burin DtPas encore d'évaluation
- Assignment: New Product Development PROJECT TITLE: Safety Alarm For Construction WorkerDocument21 pagesAssignment: New Product Development PROJECT TITLE: Safety Alarm For Construction WorkerHazim ZakiPas encore d'évaluation
- MASAR - Volume 02Document214 pagesMASAR - Volume 02Khaled MamdouhPas encore d'évaluation
- The Metabolic and Endocrine Systems NotesDocument9 pagesThe Metabolic and Endocrine Systems NotesCarl Elexer Cuyugan Ano100% (2)
- AS Chemistry Unit: 1: Topic: Periodic PropertiesDocument4 pagesAS Chemistry Unit: 1: Topic: Periodic PropertiesShoaib AhmedPas encore d'évaluation
- ASA-RAC Application GuideDocument15 pagesASA-RAC Application GuideIsrael Miranda Zamarca100% (2)
- Nuclear Power Corporation of India LimitedDocument11 pagesNuclear Power Corporation of India Limitedkevin desaiPas encore d'évaluation
- A Complete List of Books On Mead MakingDocument3 pagesA Complete List of Books On Mead MakingVictor Sá100% (1)
- Belajar Cepat Windows Server 2008Document4 pagesBelajar Cepat Windows Server 2008Faizal RasyidPas encore d'évaluation
- UTOPIAvs DYSTOPIADocument17 pagesUTOPIAvs DYSTOPIAzairaguenperaltaPas encore d'évaluation
- LR1160 SN134056 Technical Diagrams - EnglishDocument197 pagesLR1160 SN134056 Technical Diagrams - EnglishВиталий РогожинскийPas encore d'évaluation
- 390D L Excavator WAP00001-UP (MACHINE) POWERED BY C18 Engine (SEBP5236 - 43) - Sistemas y ComponentesDocument3 pages390D L Excavator WAP00001-UP (MACHINE) POWERED BY C18 Engine (SEBP5236 - 43) - Sistemas y ComponentesJuan Pablo Virreyra TriguerosPas encore d'évaluation
- AirOS 3.4 - Ubiquiti Wiki#BasicWirelessSettings#BasicWirelessSettingsDocument24 pagesAirOS 3.4 - Ubiquiti Wiki#BasicWirelessSettings#BasicWirelessSettingsAusPas encore d'évaluation
- Autism and Autism Spectrum Disorder Medical Hypothesis For Parasites Influencing AutismDocument3 pagesAutism and Autism Spectrum Disorder Medical Hypothesis For Parasites Influencing AutismCATHYPas encore d'évaluation
- DLL - Science 5 - Q3 - W2Document10 pagesDLL - Science 5 - Q3 - W2Eihcra SubacPas encore d'évaluation
- LSE100 Past Year Questions (2014/5)Document2 pagesLSE100 Past Year Questions (2014/5)Jingwen ZhangPas encore d'évaluation
- FT 180aDocument60 pagesFT 180aRobert/YG2AKR75% (4)
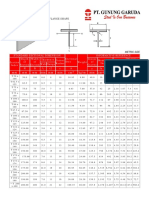
- T Beam PDFDocument2 pagesT Beam PDFjabri kotaPas encore d'évaluation