Vous aimerez peut-être aussi
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Date 1Document1 pageDate 1Muhammad Mirdho ArfiPas encore d'évaluation
- Headline Title: "Put A Quote Here To Highlight This Issue of Your Newsletter."Document3 pagesHeadline Title: "Put A Quote Here To Highlight This Issue of Your Newsletter."alexandra recimoPas encore d'évaluation
- ThanksgivingDocument1 pageThanksgivingMuhammad Mirdho ArfiPas encore d'évaluation
- Headline Title: "Put A Quote Here To Highlight This Issue of Your Newsletter."Document3 pagesHeadline Title: "Put A Quote Here To Highlight This Issue of Your Newsletter."alexandra recimoPas encore d'évaluation
- Your NameDocument1 pageYour NameMuhammad Mirdho ArfiPas encore d'évaluation
- August 22Document1 pageAugust 22rahulkmarPas encore d'évaluation
- Street Address City, ST ZIP CodeDocument1 pageStreet Address City, ST ZIP CodeMuhammad Mirdho ArfiPas encore d'évaluation
- August 22Document1 pageAugust 22rahulkmarPas encore d'évaluation
- Date 1Document1 pageDate 1Muhammad Mirdho ArfiPas encore d'évaluation
- Event Title: 1.select The Menu Content. AppetizerDocument1 pageEvent Title: 1.select The Menu Content. AppetizerMuhammad Mirdho ArfiPas encore d'évaluation
- Brosur WkakakahhsgggaaDocument4 pagesBrosur WkakakahhsgggaaDiko AprilioPas encore d'évaluation
- Brosur WkakakahhsgggaaDocument4 pagesBrosur WkakakahhsgggaaDiko AprilioPas encore d'évaluation
- 7Document2 pages7BM PannaPas encore d'évaluation
- Resume for Marketing CoordinatorDocument1 pageResume for Marketing CoordinatorArbi Yuda PamungkasPas encore d'évaluation
- Business Contact Listing TemplateDocument1 pageBusiness Contact Listing TemplateMuhammad Mirdho ArfiPas encore d'évaluation
- February 26Document2 pagesFebruary 26Muhammad Mirdho ArfiPas encore d'évaluation
- To Do List: Priority DUE Date What WHO IN Progress DoneDocument1 pageTo Do List: Priority DUE Date What WHO IN Progress DoneMuhammad Mirdho ArfiPas encore d'évaluation
- KP 3.2.6.6 NeuropathyDocument86 pagesKP 3.2.6.6 NeuropathyMuhammad Mirdho ArfiPas encore d'évaluation
- SkillsDocument1 pageSkillsAsrul MaiwaPas encore d'évaluation
- Elementary School CertificateDocument1 pageElementary School CertificateyinyangshenPas encore d'évaluation
- Tuesday Thursday Saturday: NotesDocument1 pageTuesday Thursday Saturday: NotesMuhammad Mirdho ArfiPas encore d'évaluation
- Summer Splash: CelebrationDocument1 pageSummer Splash: CelebrationKristel Eunice Fabián CristóbalPas encore d'évaluation
- Gift CertificateDocument1 pageGift CertificateMuhammad Mirdho ArfiPas encore d'évaluation
- Come Celebrate! Is Turning: (NAME)Document1 pageCome Celebrate! Is Turning: (NAME)Николче МитриќевскиPas encore d'évaluation
- KP 3.2.5.4 Rachitis - Vit D Ricketsia - OsteomalaciaDocument72 pagesKP 3.2.5.4 Rachitis - Vit D Ricketsia - OsteomalaciaMuhammad Mirdho ArfiPas encore d'évaluation
- Gift CertificateDocument1 pageGift CertificateMuhammad Mirdho ArfiPas encore d'évaluation
- Tek 9Document1 pageTek 9Iya CordilleraPas encore d'évaluation
- Your Name: Objective ExperienceDocument1 pageYour Name: Objective ExperienceAldo Christianto FernandoPas encore d'évaluation
- Your Name: ExperienceDocument1 pageYour Name: ExperienceMuhammad Mirdho ArfiPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
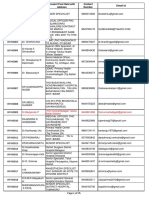
- Contact details of medical officers in KarnatakaDocument25 pagesContact details of medical officers in KarnatakaShweta jain100% (1)
- Telemedicine PPT 1Document18 pagesTelemedicine PPT 1Rikky AbdulPas encore d'évaluation
- CV Moiz Ul Haq HasmiDocument1 pageCV Moiz Ul Haq HasmiMoiz Ul Haq HashmiPas encore d'évaluation
- Irene Diamond TKR Brochure-PrintDocument39 pagesIrene Diamond TKR Brochure-PrintTusan Sidharta100% (1)
- Acute Appendicectomy: Click To Edit Master Subtitle StyleDocument38 pagesAcute Appendicectomy: Click To Edit Master Subtitle StyleSiti Khadijah MustaphaPas encore d'évaluation
- Tarsal CoalitionDocument7 pagesTarsal CoalitionFran coPas encore d'évaluation
- Splenectomy in Dogs and Cats: Indications, Surgical Technique, and Postoperative CareDocument3 pagesSplenectomy in Dogs and Cats: Indications, Surgical Technique, and Postoperative CareBeratha MuktiPas encore d'évaluation
- Total Shoulder Arthroplasty, An Overview, Indicatins and Prosthetic OptionsDocument4 pagesTotal Shoulder Arthroplasty, An Overview, Indicatins and Prosthetic OptionsYafiahnaf FirdausPas encore d'évaluation
- HNP Case Scenario For Case StudyDocument2 pagesHNP Case Scenario For Case StudyDeinielle Magdangal RomeroPas encore d'évaluation
- DENTAL IMPLANTS - ALL YOU NEED TO KNOWDocument19 pagesDENTAL IMPLANTS - ALL YOU NEED TO KNOWvishwas madaanPas encore d'évaluation
- Syntax Score Calculation SimulationDocument66 pagesSyntax Score Calculation SimulationTahari Bargas PrakosoPas encore d'évaluation
- Case ScenarioDocument1 pageCase ScenarioIrish Eunice FelixPas encore d'évaluation
- 1616823455876-Basic BRSingh Hospital Details 26th March 2021Document11 pages1616823455876-Basic BRSingh Hospital Details 26th March 2021Kiushik SarkarPas encore d'évaluation
- Osteovit: Collagen Matrix For Filling Bone DefectsDocument2 pagesOsteovit: Collagen Matrix For Filling Bone DefectsAngga SaputraPas encore d'évaluation
- Research Forehead FillerDocument5 pagesResearch Forehead FillerNavaphon ChanbangPas encore d'évaluation
- McKeown EsophagectomyDocument9 pagesMcKeown EsophagectomyDa JunPas encore d'évaluation
- Dixion EngDocument40 pagesDixion EngDennis RoblesPas encore d'évaluation
- Assessment of Pt.'s With Appendicitis by Using Nursing Care PlanDocument8 pagesAssessment of Pt.'s With Appendicitis by Using Nursing Care PlanTaate MohammedPas encore d'évaluation
- Smartmedic Million BrochureDocument11 pagesSmartmedic Million BrochureAlwin AlexanderPas encore d'évaluation
- What Does The Bible Says About The MouthDocument3 pagesWhat Does The Bible Says About The MouthAljhon DelfinPas encore d'évaluation
- Affidavit ofDocument3 pagesAffidavit ofJudeRamosPas encore d'évaluation
- Medical negligence liability cannot be establishedDocument4 pagesMedical negligence liability cannot be establishedCHANDRAKALA .B.B.Pas encore d'évaluation
- Atlas of Orthopaedic Surgical Approaches To The Lower Limbs (Rosa Ballis, Bujar H. Shabani, Dafina Bytyqi) Bibis - IrDocument88 pagesAtlas of Orthopaedic Surgical Approaches To The Lower Limbs (Rosa Ballis, Bujar H. Shabani, Dafina Bytyqi) Bibis - IrFarhan M. SalimPas encore d'évaluation
- Eaglestar Marine (S) PTE LTD Ratings SoB 3Document5 pagesEaglestar Marine (S) PTE LTD Ratings SoB 3Mazlan MohamedPas encore d'évaluation
- Abordaje Deltopectoral Vs TransdeltoideoDocument10 pagesAbordaje Deltopectoral Vs TransdeltoideoNinhoTonyOfficialPas encore d'évaluation
- Laparoscopy and Laparoscopic Surgery PDFDocument6 pagesLaparoscopy and Laparoscopic Surgery PDFIbrohim ObidovPas encore d'évaluation
- Knot Tying Manual - EthiconDocument44 pagesKnot Tying Manual - EthiconAdi Martin100% (4)
- Bone Cement PDFDocument10 pagesBone Cement PDFLee Chee SengPas encore d'évaluation
- Pediatric Patients with URI and Elective SurgeryDocument10 pagesPediatric Patients with URI and Elective SurgeryMaría Augusta Robayo UvilluzPas encore d'évaluation
- OMFS ArmamentariumDocument47 pagesOMFS ArmamentariumAdel HadyPas encore d'évaluation