Vous aimerez peut-être aussi
- Blood TransfusionDocument58 pagesBlood Transfusionmsat72100% (12)
- Blood TransfusionDocument57 pagesBlood Transfusionibzshan_Pas encore d'évaluation
- Transfusion of Blood & Blood Components1Document45 pagesTransfusion of Blood & Blood Components1Chamika Huruggamuwa100% (1)
- Surgery Slide 6 - Blood TransfusionsDocument54 pagesSurgery Slide 6 - Blood TransfusionsEman NazzalPas encore d'évaluation
- ICU Blood Transfusion & Electrolytes DisturbanceDocument26 pagesICU Blood Transfusion & Electrolytes Disturbancef6080683Pas encore d'évaluation
- Blood and Its ComponentsDocument30 pagesBlood and Its ComponentskushalPas encore d'évaluation
- Blood Transfusion ClassDocument61 pagesBlood Transfusion ClassshikhaPas encore d'évaluation
- Blood & Blood ProductsDocument126 pagesBlood & Blood ProductsdrprasadingleyPas encore d'évaluation
- Blood Components - DR. ETU-EFEOTOR T. P.Document40 pagesBlood Components - DR. ETU-EFEOTOR T. P.Princewill Seiyefa100% (1)
- Blood Grouping and BankingDocument41 pagesBlood Grouping and BankingChipego NyirendaPas encore d'évaluation
- Blood TransfusionDocument75 pagesBlood TransfusionKamal SaudPas encore d'évaluation
- Blood Transfusion TherapyDocument38 pagesBlood Transfusion TherapyAnn Merlin JobinPas encore d'évaluation
- Blood & Blood Products OnlyDocument54 pagesBlood & Blood Products OnlydrprasadingleyPas encore d'évaluation
- Blood Component Transfusion: 1st Year Pediatric ResidentDocument49 pagesBlood Component Transfusion: 1st Year Pediatric ResidentZel Azuro SolisPas encore d'évaluation
- Blood ComponenetsDocument41 pagesBlood Componenetsnighat khanPas encore d'évaluation
- Blood Components and Blood TransfusionDocument38 pagesBlood Components and Blood TransfusionjosephPas encore d'évaluation
- Blood ProductsDocument70 pagesBlood Productsjadhamade339Pas encore d'évaluation
- PPDS Rev 20 Jan 2019Document54 pagesPPDS Rev 20 Jan 2019Radinal MauludiPas encore d'évaluation
- Transfusion Medicine by Dr. Sharad JohriDocument54 pagesTransfusion Medicine by Dr. Sharad JohriShashwat JohriPas encore d'évaluation
- Surgery of Kidney Ureter and VaricoseDocument55 pagesSurgery of Kidney Ureter and VaricoseSaurabh SharmaPas encore d'évaluation
- Transfusion Medicine:: Types, Indications and ComplicationsDocument40 pagesTransfusion Medicine:: Types, Indications and ComplicationsmonichaPas encore d'évaluation
- Pediatric TransfusionDocument82 pagesPediatric TransfusionMia Lesaca-Medina100% (2)
- Serious Hazards of Transfusion: DR Kenneth S Charles MB - Bs (Uwi), FRCP (Uk), Frcpath (Uk) Senior Lecturer in HaematologyDocument65 pagesSerious Hazards of Transfusion: DR Kenneth S Charles MB - Bs (Uwi), FRCP (Uk), Frcpath (Uk) Senior Lecturer in HaematologySuneil R AlsPas encore d'évaluation
- DIC Blood Component TherapyDocument30 pagesDIC Blood Component TherapySameer KumarPas encore d'évaluation
- Blood TransfusionDocument65 pagesBlood TransfusionKate Lucernas MayugaPas encore d'évaluation
- Blood Transfusion KiranDocument34 pagesBlood Transfusion KiranKiran KumarPas encore d'évaluation
- Transfusion Medicine: DR Abdullah AnsariDocument53 pagesTransfusion Medicine: DR Abdullah AnsariFabsPas encore d'évaluation
- Blood TransfusionDocument24 pagesBlood TransfusionNerita100% (1)
- 7.hemostasis, Surgical BleedingDocument61 pages7.hemostasis, Surgical Bleedingoliyad alemayehuPas encore d'évaluation
- Transfusion of Blood and Red CellsDocument34 pagesTransfusion of Blood and Red CellsAdams Westlifer SophianoPas encore d'évaluation
- Blood TransfusionDocument22 pagesBlood TransfusionDinda KusumaPas encore d'évaluation
- Blood Products. Preparation of Blood ComponentsDocument32 pagesBlood Products. Preparation of Blood ComponentsSanthiya MadhavanPas encore d'évaluation
- Types, Indications and Complications: TransfusionDocument26 pagesTypes, Indications and Complications: TransfusionVatha NaPas encore d'évaluation
- Blood Basics1Document6 pagesBlood Basics1Celina PastorPas encore d'évaluation
- Blood Component Therapy F17Document33 pagesBlood Component Therapy F17Crystal LynaePas encore d'évaluation
- Blood and Blood ProductsDocument52 pagesBlood and Blood Productswellawalalasith100% (1)
- Blood ProductDocument35 pagesBlood Productrajan kumar100% (3)
- Blood TranfusionDocument37 pagesBlood TranfusionRaras P P100% (1)
- Transfusion Reaction - DRGSPDocument42 pagesTransfusion Reaction - DRGSPGaurav PawarPas encore d'évaluation
- Blood Transfusion in Pediatrics - Dr. RiniDocument55 pagesBlood Transfusion in Pediatrics - Dr. RiniAndyani PratiwiPas encore d'évaluation
- Blood Transfusion SeminarDocument58 pagesBlood Transfusion SeminarsharewdelelegnPas encore d'évaluation
- Blood Transfusion ProblemsDocument52 pagesBlood Transfusion ProblemsAulia RahmanPas encore d'évaluation
- Blood Component TherapyDocument13 pagesBlood Component TherapyMohamed ElgayarPas encore d'évaluation
- Blood Groups, Blood Components, Blood Transfusion PresentationDocument50 pagesBlood Groups, Blood Components, Blood Transfusion PresentationAashish Gautam100% (1)
- 6.blood Transfusion, Hemostasis & Coagulation DisordersDocument42 pages6.blood Transfusion, Hemostasis & Coagulation DisordersEyouel TadessePas encore d'évaluation
- Blood Componant Therapy (Autosaved)Document47 pagesBlood Componant Therapy (Autosaved)drkapiltPas encore d'évaluation
- Blood AdministrationDocument35 pagesBlood AdministrationnurminiePas encore d'évaluation
- BT New TemplateDocument65 pagesBT New TemplateNikky SilvestrePas encore d'évaluation
- Blood TransfusionDocument52 pagesBlood TransfusionAnonymous GC8uMx367% (3)
- Blood Products and Their UsesDocument28 pagesBlood Products and Their UsesJeevitha Vanitha100% (1)
- Blood Transfusion Guidelines - 112Document55 pagesBlood Transfusion Guidelines - 112Dhaneswara AdhyatamaPas encore d'évaluation
- HPB Adverse Transfusion ReactionDocument26 pagesHPB Adverse Transfusion ReactionFransiscus RivaldyPas encore d'évaluation
- Hemostasis and Hemotherapy - Pineda (April Rotator)Document31 pagesHemostasis and Hemotherapy - Pineda (April Rotator)Immah PinedaPas encore d'évaluation
- Blood Transfusion (3) - 123Document44 pagesBlood Transfusion (3) - 123AjeeshPas encore d'évaluation
- Rational Use of Safe BloodDocument22 pagesRational Use of Safe Bloodkamnasharma0907Pas encore d'évaluation
- 4 Component TherapyDocument50 pages4 Component TherapyJayniel MollenoPas encore d'évaluation
- 4 Blood ProductsDocument11 pages4 Blood ProductsGampa VijaykumarPas encore d'évaluation
- Disseminated Intravascular CoagulationDocument37 pagesDisseminated Intravascular CoagulationhipoclaudioPas encore d'évaluation
- Wollega University: Pre-Operation Blood Transfusion Kalkidan Muliye: Mr. Nega (Ass - Prof)Document34 pagesWollega University: Pre-Operation Blood Transfusion Kalkidan Muliye: Mr. Nega (Ass - Prof)tefesih tube ተፈስሕ ቲዮብPas encore d'évaluation
- Pre Training Discussion - BD FACSLyricDocument48 pagesPre Training Discussion - BD FACSLyricirdinamarchsyaPas encore d'évaluation
- Academic Program 2020Document2 pagesAcademic Program 2020irdinamarchsyaPas encore d'évaluation
- Permintaan Lab Disertai Ket KlinisDocument1 pagePermintaan Lab Disertai Ket KlinisirdinamarchsyaPas encore d'évaluation
- Lab Result in EnglishDocument3 pagesLab Result in EnglishirdinamarchsyaPas encore d'évaluation
- Terms of ReferenceDocument3 pagesTerms of ReferenceirdinamarchsyaPas encore d'évaluation
- Audit ToolDocument1 pageAudit ToolirdinamarchsyaPas encore d'évaluation
- 2021 Course Outline Operations Management Tutorial MTM C10Document5 pages2021 Course Outline Operations Management Tutorial MTM C10irdinamarchsyaPas encore d'évaluation
- Winter School Immuno Flyer 2020Document2 pagesWinter School Immuno Flyer 2020irdinamarchsyaPas encore d'évaluation
- Competency Are Your Staff Adequately TrainedDocument22 pagesCompetency Are Your Staff Adequately TrainedirdinamarchsyaPas encore d'évaluation
- Strengthening Regional Viral Hepatitis Laboratory CapacityDocument23 pagesStrengthening Regional Viral Hepatitis Laboratory CapacityirdinamarchsyaPas encore d'évaluation
- Competency Are Your Staff Adequately TrainedDocument22 pagesCompetency Are Your Staff Adequately TrainedirdinamarchsyaPas encore d'évaluation
- Competency Are Your Staff Adequately TrainedDocument36 pagesCompetency Are Your Staff Adequately TrainedirdinamarchsyaPas encore d'évaluation
- The Challenges and Benefit of Internal Auditing PDFDocument27 pagesThe Challenges and Benefit of Internal Auditing PDFirdinamarchsyaPas encore d'évaluation
- Manufacture of QCDocument19 pagesManufacture of QCirdinamarchsyaPas encore d'évaluation
- Antibiotik Yg Ada D RSKDDocument1 pageAntibiotik Yg Ada D RSKDirdinamarchsyaPas encore d'évaluation
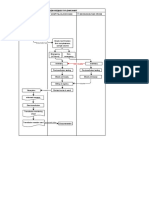
- Blood Request FlowchartDocument1 pageBlood Request FlowchartirdinamarchsyaPas encore d'évaluation
- Thesis Complete Uganda PDFDocument143 pagesThesis Complete Uganda PDFirdinamarchsyaPas encore d'évaluation
- Physicians Statement 0-2Document1 pagePhysicians Statement 0-2irdinamarchsyaPas encore d'évaluation
- BJSTR - Challenges in Early Infant Diagnosis of Beta ThalassemiaDocument4 pagesBJSTR - Challenges in Early Infant Diagnosis of Beta ThalassemiairdinamarchsyaPas encore d'évaluation
- Antibiotik Yg Ada D RSKD PDFDocument1 pageAntibiotik Yg Ada D RSKD PDFirdinamarchsyaPas encore d'évaluation
- TAT For Issuing Blood Products in EmergencyDocument4 pagesTAT For Issuing Blood Products in Emergencyirdinamarchsya100% (1)
- 01 - Current Draft WHO-CDC Biosafety RecommendationsDocument32 pages01 - Current Draft WHO-CDC Biosafety RecommendationsitsruriPas encore d'évaluation
- Uji Validasi Metode Tes Alat Hematologi Sysmex Xnl350Document1 pageUji Validasi Metode Tes Alat Hematologi Sysmex Xnl350irdinamarchsyaPas encore d'évaluation
- Use of Genexpert For Clinically Suspected MDR TBDocument6 pagesUse of Genexpert For Clinically Suspected MDR TBirdinamarchsyaPas encore d'évaluation
- Hem Lect 12 ThalassemiaDocument48 pagesHem Lect 12 ThalassemiaKholisah MardiyahPas encore d'évaluation
- Bland and Altman Plots in ExcelDocument7 pagesBland and Altman Plots in ExcelirdinamarchsyaPas encore d'évaluation
- Malignant or Benign Leukocytosis: Tracy I. GeorgeDocument10 pagesMalignant or Benign Leukocytosis: Tracy I. GeorgeirdinamarchsyaPas encore d'évaluation
- Establishment of Reference Ranges For SPE in The Pediatric Population - A. FogliDocument1 pageEstablishment of Reference Ranges For SPE in The Pediatric Population - A. FogliirdinamarchsyaPas encore d'évaluation
- Prinsip Kerja MGITDocument6 pagesPrinsip Kerja MGITirdinamarchsyaPas encore d'évaluation
- Enzymes in DigestionDocument14 pagesEnzymes in Digestionapi-188431847Pas encore d'évaluation
- Breathing TechniquesDocument26 pagesBreathing TechniquessherryPas encore d'évaluation
- Soalan Objektif Bab 10 & Bab 11Document16 pagesSoalan Objektif Bab 10 & Bab 11Sains Matematik PahangPas encore d'évaluation
- 199 Questions-Fcps Part 1 Medicine Paper - PDF 16 November 2011-By PimaDocument13 pages199 Questions-Fcps Part 1 Medicine Paper - PDF 16 November 2011-By PimaServantof Islam100% (5)
- Case Study 2Document3 pagesCase Study 2Thesa Ray PadernalPas encore d'évaluation
- Medical Terminology Cardiovascular SystemDocument35 pagesMedical Terminology Cardiovascular Systemapi-26819951486% (7)
- Penis and TesticlesDocument7 pagesPenis and TesticlesRose WidantiPas encore d'évaluation
- Janaelewis WhatispizzamadeofDocument8 pagesJanaelewis Whatispizzamadeofapi-228358375Pas encore d'évaluation
- Anatomy MCQDocument10 pagesAnatomy MCQnistaraPas encore d'évaluation
- Tetanic Contraction - WikipediaDocument9 pagesTetanic Contraction - WikipediaSIBANI CHAUDHURYPas encore d'évaluation
- Oogenesis VS SpermatogenesisDocument2 pagesOogenesis VS SpermatogenesisYousef MofiedPas encore d'évaluation
- Topographic Anatomy of Abdominal OrgansDocument18 pagesTopographic Anatomy of Abdominal OrgansHasnain IdreesPas encore d'évaluation
- Blood Supply of Head and NeckDocument42 pagesBlood Supply of Head and NeckhoneyPas encore d'évaluation
- TSH TestDocument5 pagesTSH TestdenalynPas encore d'évaluation
- Medical Terminology Chapter 1 Practice QuestionsDocument30 pagesMedical Terminology Chapter 1 Practice Questionshtb495Pas encore d'évaluation
- Preview 18041 Romano Lingual and Esthetic OrthodonticsDocument21 pagesPreview 18041 Romano Lingual and Esthetic OrthodonticsThang Nguyen TienPas encore d'évaluation
- Post Insertion Complaints and Management in Complete DenturesDocument37 pagesPost Insertion Complaints and Management in Complete Denturestribhuvan50% (2)
- Structure of Blood Vessels - StationsDocument6 pagesStructure of Blood Vessels - StationsRamya MalariniPas encore d'évaluation
- Micro Chapter 17 PPT 11th EditionDocument58 pagesMicro Chapter 17 PPT 11th EditionKartik RajputPas encore d'évaluation
- Long Bone DissectionDocument2 pagesLong Bone Dissectionapi-434212093Pas encore d'évaluation
- Aromatherapy - 600 Aromatherapy Recipes For Beauty, Health & Home - Plus Advice & Tips On How To Use Essential Oils - Nodrm PDFDocument365 pagesAromatherapy - 600 Aromatherapy Recipes For Beauty, Health & Home - Plus Advice & Tips On How To Use Essential Oils - Nodrm PDFFernanda Rodriguez75% (4)
- Ortho Intro #5 - Anchorage and HeadgearDocument5 pagesOrtho Intro #5 - Anchorage and HeadgearOrion KongPas encore d'évaluation
- LE3219 - Leather Microbiology Infection and ImmunityDocument21 pagesLE3219 - Leather Microbiology Infection and ImmunityAnik AlamPas encore d'évaluation
- BB PrelimsDocument2 pagesBB Prelimsangela verayePas encore d'évaluation
- Pharmacokinetics and Pharmacodynamics PDFDocument166 pagesPharmacokinetics and Pharmacodynamics PDFCarolina PosadaPas encore d'évaluation
- Diseases and Immunity: Defence Against MicrobesDocument55 pagesDiseases and Immunity: Defence Against MicrobesIvan Prasetya100% (1)
- Anatomy Exam 100 MARKS 04 (1) .07-1Document13 pagesAnatomy Exam 100 MARKS 04 (1) .07-1aishaalthaf.4.4Pas encore d'évaluation
- MN - B4 Revision LessonDocument34 pagesMN - B4 Revision Lessonspamzz063Pas encore d'évaluation
- Kelly Kennedy Lymphatic LessonsDocument30 pagesKelly Kennedy Lymphatic LessonsPatriciaPedroGomes100% (8)
- Pranic HealingDocument7 pagesPranic HealingArvind GuptaPas encore d'évaluation