Vous aimerez peut-être aussi
- QuizletDocument37 pagesQuizletnaimPas encore d'évaluation
- QuizletDocument118 pagesQuizletnaimPas encore d'évaluation
- QuizletDocument5 pagesQuizletnaimPas encore d'évaluation
- QuizletDocument8 pagesQuizletnaimPas encore d'évaluation
- Step 2 CS Differential DiagnosesDocument4 pagesStep 2 CS Differential DiagnosesnaimPas encore d'évaluation
- Phentermine: Anesthesiology KeywordsDocument5 pagesPhentermine: Anesthesiology KeywordsnaimPas encore d'évaluation
- QuizletDocument9 pagesQuizletnaimPas encore d'évaluation
- QuizletDocument16 pagesQuizletnaimPas encore d'évaluation
- Gastroenteritis 15Document2 pagesGastroenteritis 15naimPas encore d'évaluation
- Avery 11900 Plastic Insertable Divider 5 TabDocument1 pageAvery 11900 Plastic Insertable Divider 5 TabnaimPas encore d'évaluation
- Gastroenteritis 8Document2 pagesGastroenteritis 8naimPas encore d'évaluation
- IMPORTANT! Please Use Our New Domain Name: Irritable, Daycare Children With Same SymptomsDocument2 pagesIMPORTANT! Please Use Our New Domain Name: Irritable, Daycare Children With Same SymptomsnaimPas encore d'évaluation
- Gastroenteritis 11Document2 pagesGastroenteritis 11naimPas encore d'évaluation
- Avery 8161 Easy Peel Address LabelsDocument1 pageAvery 8161 Easy Peel Address LabelsnaimPas encore d'évaluation
- MsmmssDocument3 pagesMsmmssnaimPas encore d'évaluation
- Avery 5165 Full Sheet Shipping LabelsDocument1 pageAvery 5165 Full Sheet Shipping LabelsnaimPas encore d'évaluation
- Cardio InternetDocument46 pagesCardio InternetnaimPas encore d'évaluation
- Patoma Goldjan Uworld RewievDocument41 pagesPatoma Goldjan Uworld RewievnaimPas encore d'évaluation
- Cardio InternetDocument46 pagesCardio InternetnaimPas encore d'évaluation
- Avery 11900 Plastic Insertable Divider 5 TabDocument1 pageAvery 11900 Plastic Insertable Divider 5 TabnaimPas encore d'évaluation
- Quizlet (23) QQQQQDocument3 pagesQuizlet (23) QQQQQnaimPas encore d'évaluation
- QuizletDocument6 pagesQuizletnaimPas encore d'évaluation
- QuizletDocument6 pagesQuizletnaimPas encore d'évaluation
- Thrombotic MicroangiopathyDocument3 pagesThrombotic MicroangiopathynaimPas encore d'évaluation
- Writing Letters of RecommendationDocument4 pagesWriting Letters of Recommendationwenskyrose1100% (1)
- QuizletDocument33 pagesQuizletnaimPas encore d'évaluation
- QuizletDocument4 pagesQuizletnaimPas encore d'évaluation
- QuizletDocument5 pagesQuizletnaimPas encore d'évaluation
- Algorithms Pap CytologyDocument10 pagesAlgorithms Pap CytologynaimPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Ectopic PregnancyDocument52 pagesEctopic Pregnancybhakta100% (2)
- Case Aravind Eye Care SystemDocument4 pagesCase Aravind Eye Care Systemanon_478186565Pas encore d'évaluation
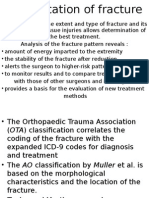
- Classification of FracturesDocument9 pagesClassification of FracturesazkaparobiPas encore d'évaluation
- Director of Pharmacy, Clinical PharmacistDocument3 pagesDirector of Pharmacy, Clinical Pharmacistapi-77860855Pas encore d'évaluation
- Cinical Duty Student Orientation Outline (N-109 MCN 2 RLE)Document2 pagesCinical Duty Student Orientation Outline (N-109 MCN 2 RLE)Krizelle MesinaPas encore d'évaluation
- Anatomy 2022Document7 pagesAnatomy 2022Rayane NaegelsPas encore d'évaluation
- Assessment of Growth and DevelopmentDocument29 pagesAssessment of Growth and DevelopmentKrupa JyothirmaiPas encore d'évaluation
- Human Sexual Response CycleDocument6 pagesHuman Sexual Response CycleAbdAllah El SaydPas encore d'évaluation
- NauseaDocument12 pagesNauseakazakom100% (2)
- Dmagette Nursing Resume 2020Document2 pagesDmagette Nursing Resume 2020api-561062694Pas encore d'évaluation
- Allied HospitalDocument6 pagesAllied HospitalMalik Mubeen 007Pas encore d'évaluation
- B1 Reading Comprehension With KeyDocument12 pagesB1 Reading Comprehension With Keyyeyes100% (33)
- ADMISSIONDocument28 pagesADMISSIONDewi AyuPas encore d'évaluation
- Directory of HSP Referral Facilities in Metro ManilaDocument2 pagesDirectory of HSP Referral Facilities in Metro ManilaWilhelmina EspejoPas encore d'évaluation
- Hypertension in PregnancyDocument68 pagesHypertension in PregnancyAbdul MoizPas encore d'évaluation
- Ovarian Dysgerminomas Pathology Overview of Ovarian DysgerminomasDocument7 pagesOvarian Dysgerminomas Pathology Overview of Ovarian DysgerminomasDevi SyamPas encore d'évaluation
- Governments Worldwide Put Emergency Contraception Into Women's HandsDocument20 pagesGovernments Worldwide Put Emergency Contraception Into Women's HandsBlimeyPas encore d'évaluation
- AmalgamDocument3 pagesAmalgamMira AnggrianiPas encore d'évaluation
- Medical Contact List of Lahore 2015Document6 pagesMedical Contact List of Lahore 2015Nida RazzaqPas encore d'évaluation
- Journey of The First 1000 Days 25 - 04 - 2018 For Web (Low Res) PDFDocument177 pagesJourney of The First 1000 Days 25 - 04 - 2018 For Web (Low Res) PDFchandraprakash_shuklPas encore d'évaluation
- General Anaesthesia: Adityadeb Ghosh B. Pharm Guru Nanak Institute of Pharmaceutical Science and Technology, Kolkata, INDocument19 pagesGeneral Anaesthesia: Adityadeb Ghosh B. Pharm Guru Nanak Institute of Pharmaceutical Science and Technology, Kolkata, INSunetraPas encore d'évaluation
- Antepartum Risk Factors For Postpartum Depression - A Follow Up Study Among Urban Women Living in Nairobi, KenyaDocument8 pagesAntepartum Risk Factors For Postpartum Depression - A Follow Up Study Among Urban Women Living in Nairobi, Kenyakartini ciatawiPas encore d'évaluation
- Urogenital Imejing: DR - Ali Imran Lubis SP - RadDocument16 pagesUrogenital Imejing: DR - Ali Imran Lubis SP - RadPutri Sari SeptirianiPas encore d'évaluation
- Regional AnesthesiaDocument4 pagesRegional AnesthesiaRisha Ethel G. BerondoPas encore d'évaluation
- Triage in The Emergency Department With PostersDocument27 pagesTriage in The Emergency Department With PostersSoleh RamlyPas encore d'évaluation
- CV Gatot Eamsc 2009Document3 pagesCV Gatot Eamsc 2009ShofaajiPas encore d'évaluation
- Requirements1&2 POdDocument10 pagesRequirements1&2 POdCJ AngelesPas encore d'évaluation
- Ingram FilingDocument29 pagesIngram FilingRoy S. JohnsonPas encore d'évaluation
- K - 7 Atrial Flutter (IKA)Document8 pagesK - 7 Atrial Flutter (IKA)thomasfelixPas encore d'évaluation
- GOPD CLINIC TIMINGS - APRIL 2022 (Tel. No. 26845900-09)Document2 pagesGOPD CLINIC TIMINGS - APRIL 2022 (Tel. No. 26845900-09)aPas encore d'évaluation