Vous aimerez peut-être aussi
- A Visual Guide To ECG Interpretation 2e 40 Jan 1 2017 41 40 1496321537 41 40 LWW 41Document1 578 pagesA Visual Guide To ECG Interpretation 2e 40 Jan 1 2017 41 40 1496321537 41 40 LWW 41xtinePas encore d'évaluation
- SoCal's UW Step 2 CK EOs (UTD 10 Nov)Document292 pagesSoCal's UW Step 2 CK EOs (UTD 10 Nov)JJ0% (1)
- Chapter 17 INTERPRETING ELECROCARDIOGRAMDocument7 pagesChapter 17 INTERPRETING ELECROCARDIOGRAMZahra Margrette SchuckPas encore d'évaluation
- Defibrillation - E-Learning Quiz 1. Identify The RhythmDocument3 pagesDefibrillation - E-Learning Quiz 1. Identify The RhythmBalaji Chinnasami100% (1)
- Divine Intervention Step 2CK Podcasts Notes - Read Only File - Docx (Dragged) 4Document3 pagesDivine Intervention Step 2CK Podcasts Notes - Read Only File - Docx (Dragged) 4winston1234Pas encore d'évaluation
- Tutors Short Cases 1 8 With Answers 2018Document5 pagesTutors Short Cases 1 8 With Answers 2018RayPas encore d'évaluation
- CardioDocument3 pagesCardiogeryPas encore d'évaluation
- Dr. Noto ID HandoutDocument35 pagesDr. Noto ID HandoutSoleil DaddouPas encore d'évaluation
- Usmle QuestionsDocument18 pagesUsmle QuestionsPat FellePas encore d'évaluation
- ECG Interpretations DR RPDocument109 pagesECG Interpretations DR RPArnis Putri RosyaniPas encore d'évaluation
- U.S. Preventive Services Task Force (USPSTF) Recommendations - Stats - Medbullets Step 2 - 3Document5 pagesU.S. Preventive Services Task Force (USPSTF) Recommendations - Stats - Medbullets Step 2 - 3mtataPas encore d'évaluation
- Amazing Esqs With Answers Pediatrics-ShelfDocument31 pagesAmazing Esqs With Answers Pediatrics-ShelfDrSajid BuzdarPas encore d'évaluation
- Neurology Musculoskeletal (MedicalBooksVN - Com)Document4 pagesNeurology Musculoskeletal (MedicalBooksVN - Com)Jonathan AiresPas encore d'évaluation
- Recall 20-21 JunyDocument131 pagesRecall 20-21 JunyNicole VinnikPas encore d'évaluation
- Medicine Review 2018 1Document470 pagesMedicine Review 2018 1Norjetalexis Maningo CabreraPas encore d'évaluation
- Interview Questions 2016 Draft Version 7-18-16Document6 pagesInterview Questions 2016 Draft Version 7-18-16Sisca Dwi AgustinaPas encore d'évaluation
- Epi Cheatsheet PDFDocument4 pagesEpi Cheatsheet PDFDrbee10Pas encore d'évaluation
- Uworld BiostatisticsDocument2 pagesUworld BiostatisticsКостянтин РоманівPas encore d'évaluation
- YFT IM Notes 1Document100 pagesYFT IM Notes 1AHMAD ALROWAILYPas encore d'évaluation
- Dermatology USMLE Step 1, 2 NotesDocument10 pagesDermatology USMLE Step 1, 2 NotesitzjuliiaPas encore d'évaluation
- Step 2 Clinical Knowledge (CK) : Sample Test QuestionsDocument59 pagesStep 2 Clinical Knowledge (CK) : Sample Test QuestionsmarceloabadPas encore d'évaluation
- Step 1 REVIEWDocument140 pagesStep 1 REVIEWRima HajjarPas encore d'évaluation
- 3 Comments SHELF Practice Questions Surgery USMLE Step 2 HomeDocument8 pages3 Comments SHELF Practice Questions Surgery USMLE Step 2 HomeIndy PhangurehPas encore d'évaluation
- Incorrect UWORLD Questions TemplateDocument29 pagesIncorrect UWORLD Questions TemplateFeroz RaZa SoomrOoPas encore d'évaluation
- ECG Interpretation DR - Rawan AlshreemDocument25 pagesECG Interpretation DR - Rawan AlshreemMarymii Al-sahlawiiPas encore d'évaluation
- SyncopeDocument3 pagesSyncopeanishdPas encore d'évaluation
- Surgery Pretest SummaryDocument9 pagesSurgery Pretest SummaryPrince DuPas encore d'évaluation
- DeVirglio NotesDocument77 pagesDeVirglio NotesAlvand SehatPas encore d'évaluation
- Step 2ck Important (AutoRecovered)Document101 pagesStep 2ck Important (AutoRecovered)Aishwarya SridharPas encore d'évaluation
- Obstetrics Cases by Caroline de CostaDocument9 pagesObstetrics Cases by Caroline de CostaJeffrey HingPas encore d'évaluation
- Nbme 7 Block 2 Answerr+ExplanationsDocument24 pagesNbme 7 Block 2 Answerr+ExplanationsShauki AliPas encore d'évaluation
- HY DermatologyDocument68 pagesHY DermatologyDiegoPas encore d'évaluation
- DermatologyDocument29 pagesDermatologymariana yllanesPas encore d'évaluation
- Pediatric 3 - Answers v1 (Wide)Document56 pagesPediatric 3 - Answers v1 (Wide)Humzala BashamPas encore d'évaluation
- Ethics Uworld NotesDocument3 pagesEthics Uworld NotesActeen MyoseenPas encore d'évaluation
- Alarm Symptoms of Hematoonco in Pediatrics: Dr. Cece Alfalah, M.Biomed, Sp.A (K) Pediatric Hematology and OncologyDocument22 pagesAlarm Symptoms of Hematoonco in Pediatrics: Dr. Cece Alfalah, M.Biomed, Sp.A (K) Pediatric Hematology and OncologyMuhammad ArifPas encore d'évaluation
- USMLE Step 3 ER PDFDocument12 pagesUSMLE Step 3 ER PDFlalaPas encore d'évaluation
- Picmonic USMLE Step 2 CK Study Plan 2016Document14 pagesPicmonic USMLE Step 2 CK Study Plan 2016YarnPas encore d'évaluation
- Actinic KeratosisDocument19 pagesActinic Keratosisattydoc1234Pas encore d'évaluation
- Arteriolar Dilator Decreases After Load Ejection FractionDocument1 pageArteriolar Dilator Decreases After Load Ejection FractionJack GuccionePas encore d'évaluation
- Read MeDocument1 pageRead MeJack GuccionePas encore d'évaluation
- Aquifer InternalMedicine11 - 45Document8 pagesAquifer InternalMedicine11 - 45JuliePas encore d'évaluation
- Third-Year OSCE Manual 2019-2020Document17 pagesThird-Year OSCE Manual 2019-2020Agleema AhmedPas encore d'évaluation
- My Divine Intervention Podcast DailyDocument1 pageMy Divine Intervention Podcast DailyDEEJKPas encore d'évaluation
- Passing The Boards Can USMLE and Orthopaedic PDFDocument5 pagesPassing The Boards Can USMLE and Orthopaedic PDFICH KhuyPas encore d'évaluation
- Quizlet (4) MMMMMMDocument30 pagesQuizlet (4) MMMMMMnaimPas encore d'évaluation
- Ventricular Isovolumetric Contractions: Tiara Calvo Leon, M.DDocument1 pageVentricular Isovolumetric Contractions: Tiara Calvo Leon, M.DSarah KhanPas encore d'évaluation
- 19 Questions and AnswersDocument144 pages19 Questions and AnswersKolusu PoojaPas encore d'évaluation
- Psych Notes For The ShelfDocument1 pagePsych Notes For The Shelfbostickdrew16Pas encore d'évaluation
- Step 1 UW Objectives Subjectwise 2022Document474 pagesStep 1 UW Objectives Subjectwise 2022saranya sankarPas encore d'évaluation
- Step1 6week DIT StudyPlan 3 PDFDocument2 pagesStep1 6week DIT StudyPlan 3 PDFSubika HaiderPas encore d'évaluation
- Deepak Step 2 CK UwDocument347 pagesDeepak Step 2 CK Uwusmleaddict proPas encore d'évaluation
- Step2 2002 Answers PDFDocument87 pagesStep2 2002 Answers PDFZioFalzPas encore d'évaluation
- Objectives IMDocument104 pagesObjectives IMlaraPas encore d'évaluation
- MGH/HMS Internal Medicine Comprehensive Review and Update Renal Cases - June 2021Document49 pagesMGH/HMS Internal Medicine Comprehensive Review and Update Renal Cases - June 2021Churschmann SpiralPas encore d'évaluation
- Brunner Step 2 CK Study PlanDocument2 pagesBrunner Step 2 CK Study PlanhellayeahPas encore d'évaluation
- Infectious DiseaseDocument28 pagesInfectious DiseaseAnukriti MamgainPas encore d'évaluation
- Aquifer InternalMedicine09 - 55Document7 pagesAquifer InternalMedicine09 - 55JuliePas encore d'évaluation
- Yunisa Hasna Hanafi: Committee of SponsorshipDocument1 pageYunisa Hasna Hanafi: Committee of SponsorshipNur akilaPas encore d'évaluation
- Syafira Nofwanda: Committee of SponsorshipDocument1 pageSyafira Nofwanda: Committee of SponsorshipNur akilaPas encore d'évaluation
- GD3. Normal ChildOKDocument22 pagesGD3. Normal ChildOKArinta AtmasariPas encore d'évaluation
- Blok 22 - Skenario D - 2019 Neonatal Case: ST TH THDocument6 pagesBlok 22 - Skenario D - 2019 Neonatal Case: ST TH THNur akilaPas encore d'évaluation
- Fidia Paramitha Putri: Committee of FundraisingDocument1 pageFidia Paramitha Putri: Committee of FundraisingNur akilaPas encore d'évaluation
- Leo Medianto Faziqin: Committee of FundraisingDocument1 pageLeo Medianto Faziqin: Committee of FundraisingNur akilaPas encore d'évaluation
- M. Wika Kurniawan: Committee of FundraisingDocument1 pageM. Wika Kurniawan: Committee of FundraisingNur akilaPas encore d'évaluation
- Mita Al-Maida: Committee of FundraisingDocument1 pageMita Al-Maida: Committee of FundraisingNur akilaPas encore d'évaluation
- Skenario C Blok 15 Tahun 2018Document5 pagesSkenario C Blok 15 Tahun 2018Nur akilaPas encore d'évaluation
- M. Wika Kurniawan: Committee of FundraisingDocument1 pageM. Wika Kurniawan: Committee of FundraisingNur akilaPas encore d'évaluation
- Junoretta: Committee of FundraisingDocument1 pageJunoretta: Committee of FundraisingNur akilaPas encore d'évaluation
- Andrew Fabian: Committee of FundraisingDocument1 pageAndrew Fabian: Committee of FundraisingNur akilaPas encore d'évaluation
- Reihan Putri Awaliah: Committee of SponsorshipDocument1 pageReihan Putri Awaliah: Committee of SponsorshipNur akilaPas encore d'évaluation
- Muhammad Nur Richard S.: Committee of FundraisingDocument1 pageMuhammad Nur Richard S.: Committee of FundraisingNur akilaPas encore d'évaluation
- Nurlaili Maya: Committee of SponsorshipDocument1 pageNurlaili Maya: Committee of SponsorshipNur akilaPas encore d'évaluation
- Muhammad Nur Richard S.: Committee of FundraisingDocument1 pageMuhammad Nur Richard S.: Committee of FundraisingNur akilaPas encore d'évaluation
- Absen Panitia SporaDocument10 pagesAbsen Panitia SporaNur akilaPas encore d'évaluation
- Skenario B Blok 15 Kelompok DUA (Sementara)Document8 pagesSkenario B Blok 15 Kelompok DUA (Sementara)Nur akilaPas encore d'évaluation
- Cipta Jaya Setiawan: Committee of FundraisingDocument1 pageCipta Jaya Setiawan: Committee of FundraisingNur akilaPas encore d'évaluation
- Jadwal Blok 14tahun 2018Document10 pagesJadwal Blok 14tahun 2018Nur akilaPas encore d'évaluation
- Bahan LIDocument22 pagesBahan LINur akilaPas encore d'évaluation
- Anggun Permata Sari: CommitteeDocument1 pageAnggun Permata Sari: CommitteeNur akilaPas encore d'évaluation
- 14 HF-Limfoma GI TractDocument27 pages14 HF-Limfoma GI TractNur akilaPas encore d'évaluation
- 12 RLDDocument43 pages12 RLDNur akilaPas encore d'évaluation
- Treatment of Tuberculosis: Zen Ahmad Medical Faculty, Sriwijaya UniversityDocument46 pagesTreatment of Tuberculosis: Zen Ahmad Medical Faculty, Sriwijaya UniversityNur akilaPas encore d'évaluation
- Analisis Masalah Tutorial KeduaDocument7 pagesAnalisis Masalah Tutorial KeduaNur akilaPas encore d'évaluation
- Blok 8 Skenario A 2016Document5 pagesBlok 8 Skenario A 2016Nur akilaPas encore d'évaluation
- Skenario B Blok 14 Tahun 2018Document5 pagesSkenario B Blok 14 Tahun 2018Nur akilaPas encore d'évaluation
- Pulmonary Rehabilitation: Nyimas FatimahDocument61 pagesPulmonary Rehabilitation: Nyimas FatimahNur akilaPas encore d'évaluation
- 12 RLDDocument43 pages12 RLDNur akilaPas encore d'évaluation
- Bos Specialty Assignment Cardiology-AmbroseDocument11 pagesBos Specialty Assignment Cardiology-Ambroseapi-396965096Pas encore d'évaluation
- ECG, EEG &, EMG: 45 Notes To PGDocument6 pagesECG, EEG &, EMG: 45 Notes To PGskycall28Pas encore d'évaluation
- WSDDocument13 pagesWSDhinatakunhinata75Pas encore d'évaluation
- VSD 180207074930Document33 pagesVSD 180207074930widyaPas encore d'évaluation
- Heart Valve DiseaseDocument67 pagesHeart Valve DiseaseSaba SivaPas encore d'évaluation
- WS Emergency Echo SYMCARD 2022Document33 pagesWS Emergency Echo SYMCARD 2022IndRa KaBhuomPas encore d'évaluation
- Post PCI Care When To ReferDocument25 pagesPost PCI Care When To ReferRahmat HidayatullahPas encore d'évaluation
- Cardiology MnemonicDocument46 pagesCardiology MnemonicA.h.Murad100% (1)
- VT Ventricular TachyDocument1 pageVT Ventricular Tachymadimadi11Pas encore d'évaluation
- Acs OsceDocument4 pagesAcs OsceYohanes ArviPas encore d'évaluation
- Types of Cardiac ArrhythmiasDocument2 pagesTypes of Cardiac ArrhythmiasDomingo, Viella Clarisse S.Pas encore d'évaluation
- LP UapDocument18 pagesLP UapHat MutisalPas encore d'évaluation
- 2007 Electrocardiographic Manifestations Pediatric EcgDocument10 pages2007 Electrocardiographic Manifestations Pediatric EcgAngel NspPas encore d'évaluation
- AntiArrhythmic DrugsDocument7 pagesAntiArrhythmic DrugsKAZI RAHATPas encore d'évaluation
- Board Desember 2015 Fix Answer - BALIDocument67 pagesBoard Desember 2015 Fix Answer - BALIrahageng wida kusuma100% (1)
- Atrial Septal DefectDocument1 pageAtrial Septal DefectChlo14Pas encore d'évaluation
- Pulseless Arrest Algorithm For Managing VF and Pulseless VTDocument3 pagesPulseless Arrest Algorithm For Managing VF and Pulseless VTLaili CinthiaPas encore d'évaluation
- Mitral Stenosis AnDocument14 pagesMitral Stenosis AnCynthia wilsonPas encore d'évaluation
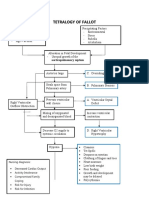
- Concept Map Tetralogy of FallotDocument2 pagesConcept Map Tetralogy of FallotKarl KiwisPas encore d'évaluation
- Final Sheet MotalityDocument69 pagesFinal Sheet MotalityAshima GabgotraPas encore d'évaluation
- 1 JurnalDocument4 pages1 JurnalKadek MahariniPas encore d'évaluation
- Dilated Cardiomyopathy Notes AtfDocument15 pagesDilated Cardiomyopathy Notes AtfSingha ChangsiriwatanaPas encore d'évaluation
- Hi-Yield Notes in Im & PediaDocument20 pagesHi-Yield Notes in Im & PediaJohn Christopher LucesPas encore d'évaluation
- Programma S PriglasheniemDocument2 pagesProgramma S PriglasheniemAhmed AhmedPas encore d'évaluation
- Heart SoundsDocument20 pagesHeart Soundsshd9617Pas encore d'évaluation
- Checklist - Monitor - EKG TechDocument5 pagesChecklist - Monitor - EKG TechATPas encore d'évaluation