Vous aimerez peut-être aussi
- OBESITY - Cayce Health DatabaseDocument4 pagesOBESITY - Cayce Health Databasewcwjr55Pas encore d'évaluation
- Unmeet Need Is LDL-C Lowering When Regular Statin Wont DoDocument40 pagesUnmeet Need Is LDL-C Lowering When Regular Statin Wont Doyan salvianto100% (1)
- Treatment Based On: Pathophysiology of HyperglycemiaDocument38 pagesTreatment Based On: Pathophysiology of HyperglycemiaRoby KieranPas encore d'évaluation
- Intraocular Pressure and Aqueous Humor DynamicsDocument36 pagesIntraocular Pressure and Aqueous Humor DynamicsIntan EkarulitaPas encore d'évaluation
- Dyslipdiemia 2022Document75 pagesDyslipdiemia 2022LeePas encore d'évaluation
- A656 GR 80 Brochure 06-26-08Document2 pagesA656 GR 80 Brochure 06-26-08OsmanPas encore d'évaluation
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919Pas encore d'évaluation
- Chemistry DemosDocument170 pagesChemistry DemosStacey BensonPas encore d'évaluation
- NCP Ineffective Breathing ActualDocument3 pagesNCP Ineffective Breathing ActualArian May Marcos100% (1)
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibPas encore d'évaluation
- Understanding The Needs of The High Productive DyslipidemiaDocument47 pagesUnderstanding The Needs of The High Productive DyslipidemiachchchchkPas encore d'évaluation
- Intensity of Cholesterol Lowering With Statin in PatientsDocument23 pagesIntensity of Cholesterol Lowering With Statin in Patientsandri ansyahPas encore d'évaluation
- 2017 DCP 1. Telmisartan Untuk KasusDocument26 pages2017 DCP 1. Telmisartan Untuk KasusOcto IndradjajaPas encore d'évaluation
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibPas encore d'évaluation
- Global Risk of Cardiovascular Disease: Assessment and ApplicationDocument18 pagesGlobal Risk of Cardiovascular Disease: Assessment and ApplicationEmdan SengadjiPas encore d'évaluation
- What's New in Lipid GuidelinesDocument31 pagesWhat's New in Lipid GuidelinesYunita WidyaningsihPas encore d'évaluation
- Raza2004 PDFDocument12 pagesRaza2004 PDFIvana RuseskaPas encore d'évaluation
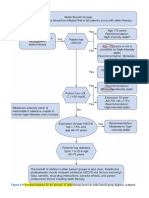
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارPas encore d'évaluation
- Materi Hipertensi Dr. Irma W, SP - PDDocument56 pagesMateri Hipertensi Dr. Irma W, SP - PDFina Syahrotul AdzimahPas encore d'évaluation
- Managing Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoDocument45 pagesManaging Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoaprinaaaPas encore d'évaluation
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919Pas encore d'évaluation
- 27 FullDocument6 pages27 FullKrishna R KhanalPas encore d'évaluation
- Statins and Beyond Concurrent Strategies For Prevention of Cardiovascular Disease in Patients WiDocument17 pagesStatins and Beyond Concurrent Strategies For Prevention of Cardiovascular Disease in Patients WiMamad TrihatmowidjoyoPas encore d'évaluation
- Jos 2021 01249jdfhjdsDocument13 pagesJos 2021 01249jdfhjdsAnonymous tG35SYROzEPas encore d'évaluation
- Management of Blood Cholesterol 2019Document2 pagesManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassPas encore d'évaluation
- Original Article: Journal of Clinical Lipidology (2017)Document12 pagesOriginal Article: Journal of Clinical Lipidology (2017)IrhamPas encore d'évaluation
- How Should One Decide Whom To Treat For Hypertension?: Jay N. Cohn, M.DDocument33 pagesHow Should One Decide Whom To Treat For Hypertension?: Jay N. Cohn, M.DAn-Nisa Khoirun UmmiPas encore d'évaluation
- Dislipid 2 PDFDocument4 pagesDislipid 2 PDFWahyuningsih HamidPas encore d'évaluation
- Association of Blood Pressure Control and Metabolic Syndrome With Cardiovascular Risk in Elderly Japanese: JATOS StudyDocument7 pagesAssociation of Blood Pressure Control and Metabolic Syndrome With Cardiovascular Risk in Elderly Japanese: JATOS StudyRobertoPas encore d'évaluation
- Diabetes and Vascular Disease Research 2010 Younis 289 95Document8 pagesDiabetes and Vascular Disease Research 2010 Younis 289 95Marthin HotangPas encore d'évaluation
- Asap LipidDocument131 pagesAsap LipidagassiPas encore d'évaluation
- HypertensionDocument8 pagesHypertensionchandra9000Pas encore d'évaluation
- Edit Virtual HR Managing Dyslipidemia in Special PopulationDocument38 pagesEdit Virtual HR Managing Dyslipidemia in Special PopulationIkmah FauzanPas encore d'évaluation
- RosuvastatinDocument62 pagesRosuvastatinEileen del RosarioPas encore d'évaluation
- Ann Soehee - Tctap2021 - SPCDocument43 pagesAnn Soehee - Tctap2021 - SPCSaad KhanPas encore d'évaluation
- 3 - Statin Primary Secondary MelaDocument57 pages3 - Statin Primary Secondary MelaKurniadin YayanPas encore d'évaluation
- Moriyama Dan Takahashi, 2016.Document12 pagesMoriyama Dan Takahashi, 2016.Jeje MystearicaPas encore d'évaluation
- 593 Full PDFDocument11 pages593 Full PDFsalman672003Pas encore d'évaluation
- Lecture 25 - Plasma Ins 3 - 2006Document31 pagesLecture 25 - Plasma Ins 3 - 2006api-3703352Pas encore d'évaluation
- Dyslipidemia 2018Document8 pagesDyslipidemia 2018R JannahPas encore d'évaluation
- Dyslipidaemias 2019Document30 pagesDyslipidaemias 2019Adinda DianPas encore d'évaluation
- Cardiometabolic Syndrome: & DR Dhafir A. MahmoodDocument62 pagesCardiometabolic Syndrome: & DR Dhafir A. MahmoodJacob AlphaPas encore d'évaluation
- Atorvastatin Statin in CVD ManagementDocument37 pagesAtorvastatin Statin in CVD ManagementSriPas encore d'évaluation
- Statins in CVD Management: Is Just Lipid Lowering Enough?Document37 pagesStatins in CVD Management: Is Just Lipid Lowering Enough?SriPas encore d'évaluation
- Slide Curriculum Diabetes and CardiologyDocument52 pagesSlide Curriculum Diabetes and CardiologyNazmul Hasan MahmudPas encore d'évaluation
- Dyslipidemia - Diabetes Mellitus - Cardiovascular Risk StratificationDocument27 pagesDyslipidemia - Diabetes Mellitus - Cardiovascular Risk StratificationryndaPas encore d'évaluation
- New Developments in The Management of DyslipidemiaDocument63 pagesNew Developments in The Management of DyslipidemiaM Azmi HPas encore d'évaluation
- Journal of Diabetes and Its ComplicationsDocument6 pagesJournal of Diabetes and Its ComplicationsNadia Rezky ElizaPas encore d'évaluation
- Roseday EZ Webinar SlidesDocument35 pagesRoseday EZ Webinar SlidesPragnesh ShahPas encore d'évaluation
- Dyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDDocument15 pagesDyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيارPas encore d'évaluation
- Diabetes Manejo DislipidemiaDocument8 pagesDiabetes Manejo DislipidemiaLuis C Ribon VPas encore d'évaluation
- 2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"Document51 pages2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"dr_yasserPas encore d'évaluation
- DM RSMD (Dr. Andi Sulistyo H, SP - PD)Document54 pagesDM RSMD (Dr. Andi Sulistyo H, SP - PD)desyPas encore d'évaluation
- Dyslipidaemia 2019Document61 pagesDyslipidaemia 2019fatima.shqeratPas encore d'évaluation
- Jurnal 4 WordDocument20 pagesJurnal 4 WordSri MaryatiPas encore d'évaluation
- Metabolic Syndrome, Diabetes, and Cardiovascular Disease: Implications For Preventive CardiologyDocument36 pagesMetabolic Syndrome, Diabetes, and Cardiovascular Disease: Implications For Preventive CardiologyAlvianridersPas encore d'évaluation
- CVD in Diabetes - EADSG 2016Document57 pagesCVD in Diabetes - EADSG 2016OmarPas encore d'évaluation
- LDL InggDocument7 pagesLDL InggDuti AprilniPas encore d'évaluation
- Aztor Cme NewDocument59 pagesAztor Cme NewSheikh Sharfuddin RajeevPas encore d'évaluation
- Lower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsDocument59 pagesLower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsJamsidul Hassan RajibPas encore d'évaluation
- Applicability of Recent Dyslipidemia Guidelines in Clinical PracticeDocument4 pagesApplicability of Recent Dyslipidemia Guidelines in Clinical PracticeDokter FebyanPas encore d'évaluation
- Preventing Cardiovascular Disease in Patients With.2 PDFDocument3 pagesPreventing Cardiovascular Disease in Patients With.2 PDFbacharelado2010Pas encore d'évaluation
- Baseline Low-Density LipoproteinDocument9 pagesBaseline Low-Density LipoproteinjoPas encore d'évaluation
- TB and Lung CancerDocument26 pagesTB and Lung CanceraprinaaaPas encore d'évaluation
- Managing Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoDocument45 pagesManaging Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoaprinaaaPas encore d'évaluation
- 4.release How To Intensify Basal Insulin With Premix and Basal Bolus ApproachDocument42 pages4.release How To Intensify Basal Insulin With Premix and Basal Bolus ApproachaprinaaaPas encore d'évaluation
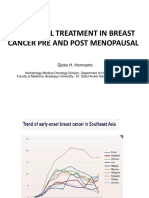
- Breast Cancer - ETDocument21 pagesBreast Cancer - ETaprinaaaPas encore d'évaluation
- Bpjs Insulin 2015Document34 pagesBpjs Insulin 2015aprinaaaPas encore d'évaluation
- Tatalaksana Dan Titrasi InsulinDocument34 pagesTatalaksana Dan Titrasi InsulinaprinaaaPas encore d'évaluation
- Hypertension. Pengendalian Faktor Risiko Penyakit Kardiovaskular DINKES TK 1 BJM 23 Maret 2016Document38 pagesHypertension. Pengendalian Faktor Risiko Penyakit Kardiovaskular DINKES TK 1 BJM 23 Maret 2016aprinaaaPas encore d'évaluation
- Non Biliary PancreatitisDocument9 pagesNon Biliary PancreatitisaprinaaaPas encore d'évaluation
- Mon AnhDocument7 pagesMon AnhDavid NguyenPas encore d'évaluation
- Impact of Job Design On Employee Engagement: A Theoretical and Literature ReviewDocument6 pagesImpact of Job Design On Employee Engagement: A Theoretical and Literature ReviewAnonymous CwJeBCAXpPas encore d'évaluation
- EESC 111 Worksheets Module 5Document5 pagesEESC 111 Worksheets Module 5Keira O'HowPas encore d'évaluation
- Qualitative Tests Organic NotesDocument5 pagesQualitative Tests Organic NotesAdorned. pearlPas encore d'évaluation
- Epoxy Data - AF35LVE TDS - ED4 - 11.17Document8 pagesEpoxy Data - AF35LVE TDS - ED4 - 11.17HARESH REDDYPas encore d'évaluation
- Gratuity SlidesDocument11 pagesGratuity SlidesK V GondiPas encore d'évaluation
- Oral Rehydration SolutionDocument22 pagesOral Rehydration SolutionAlkaPas encore d'évaluation
- Shoulder Joint Position Sense Improves With ElevationDocument10 pagesShoulder Joint Position Sense Improves With ElevationpredragbozicPas encore d'évaluation
- 7 LevelDocument5 pages7 LevelACHREF RIHANIPas encore d'évaluation
- 1 A Finalexam FNH330 June 2015 Final Review QuestionsDocument6 pages1 A Finalexam FNH330 June 2015 Final Review QuestionsChinley HinacayPas encore d'évaluation
- Biology Project Cronary Heart Diseas (CHD)Document7 pagesBiology Project Cronary Heart Diseas (CHD)احمد المغربي50% (2)
- InotroposDocument4 pagesInotroposjuan camiloPas encore d'évaluation
- 1.8 SAK Conservations of Biodiversity EX-SITU in SITUDocument7 pages1.8 SAK Conservations of Biodiversity EX-SITU in SITUSandipPas encore d'évaluation
- Planificare Săptămânală - Clasa A II-a (Fairyland 2)Document6 pagesPlanificare Săptămânală - Clasa A II-a (Fairyland 2)Oxy Oxy100% (1)
- CatalogDocument12 pagesCatalogjonz afashPas encore d'évaluation
- Phoenix Contact DATA SHEETDocument16 pagesPhoenix Contact DATA SHEETShivaniPas encore d'évaluation
- TFU-Risk Assessment RA-11 - Use of Grooving & Threading MachinesDocument1 pageTFU-Risk Assessment RA-11 - Use of Grooving & Threading Machinesarshin wildanPas encore d'évaluation
- WEEK 7-8: Health 9 Module 4Document8 pagesWEEK 7-8: Health 9 Module 4Heidee BasasPas encore d'évaluation
- Unit Two The Health Benefits of Physical ActivityDocument10 pagesUnit Two The Health Benefits of Physical ActivityYoseph DefaruPas encore d'évaluation
- BDC 6566Document6 pagesBDC 6566jack.simpson.changPas encore d'évaluation
- Market Pulse Q4 Report - Nielsen Viet Nam: Prepared by Nielsen Vietnam February 2017Document8 pagesMarket Pulse Q4 Report - Nielsen Viet Nam: Prepared by Nielsen Vietnam February 2017K57.CTTT BUI NGUYEN HUONG LYPas encore d'évaluation
- Demolition/Removal Permit Application Form: Planning, Property and Development DepartmentDocument3 pagesDemolition/Removal Permit Application Form: Planning, Property and Development DepartmentAl7amdlellahPas encore d'évaluation
- Nursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDocument11 pagesNursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDa NicaPas encore d'évaluation
- BT HandoutsDocument4 pagesBT HandoutsNerinel CoronadoPas encore d'évaluation
- Report Text: General ClassificationDocument7 pagesReport Text: General Classificationrisky armala syahraniPas encore d'évaluation