Vous aimerez peut-être aussi
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtD'EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtÉvaluation : 5 sur 5 étoiles5/5 (1)
- Pa 02 CardioDocument45 pagesPa 02 CardioElly NuñezPas encore d'évaluation
- Heart Failure Slides 2024Document43 pagesHeart Failure Slides 2024b9p6vmfnc4Pas encore d'évaluation
- Innovation in Clinical Care in Heart FailureDocument107 pagesInnovation in Clinical Care in Heart FailureSebastian Henao ErazoPas encore d'évaluation
- Pathophysiology of HFDocument40 pagesPathophysiology of HFHayaPas encore d'évaluation
- HeartFailure Nursing FIK 2014Document101 pagesHeartFailure Nursing FIK 2014Putri NurlaeliPas encore d'évaluation
- Pharmacotherapy - Heart Failure - Dr. Mohammed KamalDocument62 pagesPharmacotherapy - Heart Failure - Dr. Mohammed KamalMohammed KamalPas encore d'évaluation
- CARDIOMYOPATHIESDocument46 pagesCARDIOMYOPATHIESStella CooKeyPas encore d'évaluation
- Congestive Heart Failure: Elias S. (MD+) March 2015 DBUDocument35 pagesCongestive Heart Failure: Elias S. (MD+) March 2015 DBUkikiPas encore d'évaluation
- Heart FailureDocument118 pagesHeart FailureAli Murtaza AbbasPas encore d'évaluation
- Incidence Pathophysiology Classification Causes Diagnosis Assessing Cardiovascular Disability Treatment MessagesDocument67 pagesIncidence Pathophysiology Classification Causes Diagnosis Assessing Cardiovascular Disability Treatment MessagesAhmed ElshewiPas encore d'évaluation
- HHFFDocument56 pagesHHFFNesru Ahmed AkkichuPas encore d'évaluation
- 9, CHF BestDocument43 pages9, CHF BestauPas encore d'évaluation
- Heart Failure & Cardiac Arrest: Rony YuliwansyahDocument92 pagesHeart Failure & Cardiac Arrest: Rony YuliwansyahSasha ManoPas encore d'évaluation
- Thursday Nov 3rd - BayehDocument12 pagesThursday Nov 3rd - BayehFatima MaazPas encore d'évaluation
- Internal Medicine Lecture 6 Cardiomyopathies and MyocarditidesDocument98 pagesInternal Medicine Lecture 6 Cardiomyopathies and MyocarditidesDaily MedicinePas encore d'évaluation
- Heart Failure 2019 FK Unisma RevisiDocument95 pagesHeart Failure 2019 FK Unisma RevisiMuhammad Sandy Ali YafiePas encore d'évaluation
- Heart Failure Idi SidoarjoDocument111 pagesHeart Failure Idi SidoarjoIka Kusuma WardhaniPas encore d'évaluation
- Cardiovascular HO Final GROUP2Document72 pagesCardiovascular HO Final GROUP2Siraj ShiferawPas encore d'évaluation
- Kuliah Pakar HF FKUMMDocument46 pagesKuliah Pakar HF FKUMMOkta Dwi Kusuma AyuPas encore d'évaluation
- Unit IV. Drugs For CHFDocument26 pagesUnit IV. Drugs For CHFChinenye AkwuePas encore d'évaluation
- Curs Cardiomiopatii de Prezentat 15 Dec - 2015Document194 pagesCurs Cardiomiopatii de Prezentat 15 Dec - 2015Bogdanel MihaiPas encore d'évaluation
- Diagnostico HF 2004Document8 pagesDiagnostico HF 2004Carlos Alan Lopez100% (1)
- Gagal JantungDocument69 pagesGagal JantungKota Tako100% (1)
- CARDIOMYOPATHIESDocument80 pagesCARDIOMYOPATHIESNadun MethwadanePas encore d'évaluation
- Understanding Cardiomyopathy: Causes, Symptoms and TreatmentDocument54 pagesUnderstanding Cardiomyopathy: Causes, Symptoms and TreatmentDanny DesuPas encore d'évaluation
- Heart FailureDocument6 pagesHeart FailureNinna Isabel VictorioPas encore d'évaluation
- Congestive Heart FailureDocument13 pagesCongestive Heart FailureAgeng BudianantiPas encore d'évaluation
- Heart Failure in Sub-Saharan Africa: A Clinical Approach: ReviewDocument9 pagesHeart Failure in Sub-Saharan Africa: A Clinical Approach: ReviewrizkaPas encore d'évaluation
- Management of Heart Failure: DR Ambakederemo TE Consultant Physician/cardiologist NduthDocument71 pagesManagement of Heart Failure: DR Ambakederemo TE Consultant Physician/cardiologist NduthPrincewill SeiyefaPas encore d'évaluation
- Heart Failure 1Document50 pagesHeart Failure 1dhiraj parmar100% (1)
- CARDIOMYOPATHYDocument64 pagesCARDIOMYOPATHYgalemayehu471Pas encore d'évaluation
- Curs 9 Myocarditis CardiomyopathyDocument41 pagesCurs 9 Myocarditis CardiomyopathyIliescu DenisaPas encore d'évaluation
- Heart FailureDocument94 pagesHeart FailureAnusha Verghese100% (1)
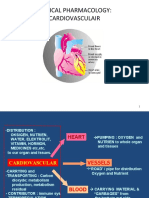
- CLINICAL PHARMACOLOGY OF CARDIOVASCULAR DRUGSDocument49 pagesCLINICAL PHARMACOLOGY OF CARDIOVASCULAR DRUGSfazry 415Pas encore d'évaluation
- Heart FailureDocument17 pagesHeart FailureIsna IndahPas encore d'évaluation
- 10 CardiomyopathyDocument71 pages10 CardiomyopathyAnonymous vUEDx8100% (5)
- Clinical Pharmacology of Cardiovascular DiseasesDocument49 pagesClinical Pharmacology of Cardiovascular DiseaseservinasetianingsihPas encore d'évaluation
- Planning: Determine Patient's Clinical StatusDocument17 pagesPlanning: Determine Patient's Clinical StatusAsti DwiningsihPas encore d'évaluation
- Cardiomyopathies: Budi Yuli Setianto Department of Cardiology Faculty of Medicine Gadjah Mada University YogyakartaDocument43 pagesCardiomyopathies: Budi Yuli Setianto Department of Cardiology Faculty of Medicine Gadjah Mada University YogyakartaadnajaniPas encore d'évaluation
- 8 - Hypertensive Vascular DiseaseDocument24 pages8 - Hypertensive Vascular DiseaseHamzehPas encore d'évaluation
- Heart Failure and CardiomyopathiesDocument26 pagesHeart Failure and Cardiomyopathieslionel andreaPas encore d'évaluation
- Hypertension: Nucleus Medical MediaDocument17 pagesHypertension: Nucleus Medical Mediakrish oswalPas encore d'évaluation
- Cme HFDocument30 pagesCme HFTze SiangPas encore d'évaluation
- Heart Failure: DR Kaem Shir AliDocument24 pagesHeart Failure: DR Kaem Shir AliMwanja MosesPas encore d'évaluation
- Pharmacotherapy of heart failureDocument79 pagesPharmacotherapy of heart failureAbera JamboPas encore d'évaluation
- Chronic Heart Failure CHFDocument11 pagesChronic Heart Failure CHFChen BrionesPas encore d'évaluation
- Congestive Heart Failure CHF: Dr. Suhaemi, SPPD, FinasimDocument94 pagesCongestive Heart Failure CHF: Dr. Suhaemi, SPPD, FinasimDella DevegaPas encore d'évaluation
- CardiomyopathyDocument8 pagesCardiomyopathyKarisaPas encore d'évaluation
- Cardiac Failure: Dr. Abdul Ghani WaseemDocument33 pagesCardiac Failure: Dr. Abdul Ghani WaseemFarwaPas encore d'évaluation
- Cardiomyopathies 6th Year Seminar GRP BBDocument42 pagesCardiomyopathies 6th Year Seminar GRP BBmohamedeen hamza100% (1)
- Systolic vs Diastolic Heart FailureDocument57 pagesSystolic vs Diastolic Heart FailureRashiden MadjalesPas encore d'évaluation
- HTN and CHFDocument29 pagesHTN and CHFkiflomPas encore d'évaluation
- Heart Failure PDFDocument25 pagesHeart Failure PDFDewMaL HealthPas encore d'évaluation
- Gagal Jantung (Prof. Dr. DR Ali Aspar M, SP - PD, SP - JP)Document45 pagesGagal Jantung (Prof. Dr. DR Ali Aspar M, SP - PD, SP - JP)Taufiq RamadhanPas encore d'évaluation
- The Clinical Epidemiology of Cardiac Disease in Chronic Renal FailureDocument10 pagesThe Clinical Epidemiology of Cardiac Disease in Chronic Renal FailureRaden Mas IkhsanPas encore d'évaluation
- Heart FailureDocument4 pagesHeart FailurersheedmahdiiPas encore d'évaluation
- Myocardial Diseases: Marvi G. Dulnuan - Niog, MD, FPSPDocument94 pagesMyocardial Diseases: Marvi G. Dulnuan - Niog, MD, FPSPLianne LagayanPas encore d'évaluation
- Pathology of Heart Failure and CardiomyopathiesDocument33 pagesPathology of Heart Failure and Cardiomyopathiesciyace7849Pas encore d'évaluation
- Gene and CVS DiseasesDocument61 pagesGene and CVS Diseasesnora almutairiPas encore d'évaluation
- Carotid Doppler Study: Dr.I.Gurubharath MD PHD DR - Pooja MDDocument116 pagesCarotid Doppler Study: Dr.I.Gurubharath MD PHD DR - Pooja MDJing CruzPas encore d'évaluation
- Core 5.1 14122017FDocument3 pagesCore 5.1 14122017FJing CruzPas encore d'évaluation
- Restrictive CardiomyopathyDocument15 pagesRestrictive CardiomyopathyJing CruzPas encore d'évaluation
- Focused Cardiac Ultrasound: Recommendations From The American Society of EchocardiographyDocument15 pagesFocused Cardiac Ultrasound: Recommendations From The American Society of EchocardiographyPaola CastellanosPas encore d'évaluation
- Credentialing Process for Sonographers in CanadaDocument1 pageCredentialing Process for Sonographers in CanadaJing CruzPas encore d'évaluation
- 5 Upper Extremity Arterial Duplex Evaluation Updated 2018 PDFDocument8 pages5 Upper Extremity Arterial Duplex Evaluation Updated 2018 PDFHasan Mohammad NayeemPas encore d'évaluation
- Phlebolymphology: Vol 28 - No. 1 - 2021 - P1-36 No. 103Document39 pagesPhlebolymphology: Vol 28 - No. 1 - 2021 - P1-36 No. 103Jing CruzPas encore d'évaluation
- 2020 in Review: A Focus On Members, An Emphasis On ActionDocument1 page2020 in Review: A Focus On Members, An Emphasis On ActionJing CruzPas encore d'évaluation
- Alternate Pathway PrerequisitesDocument1 pageAlternate Pathway PrerequisitesJing CruzPas encore d'évaluation
- Sports ScreeningDocument8 pagesSports ScreeningJing CruzPas encore d'évaluation
- A Guideline Protocol For The Diagnosis and Assessment of Marfans Syndrome From The British Society of Echocardiography Education CommitteeDocument3 pagesA Guideline Protocol For The Diagnosis and Assessment of Marfans Syndrome From The British Society of Echocardiography Education CommitteeJing CruzPas encore d'évaluation
- Mitral Valve RepairDocument5 pagesMitral Valve RepairJing CruzPas encore d'évaluation
- AIM Guidelines ArterialUltrasoundDocument20 pagesAIM Guidelines ArterialUltrasoundSmithery DiaPas encore d'évaluation
- ARVCDocument7 pagesARVCJing CruzPas encore d'évaluation
- Vascular Technology Content OutlineDocument5 pagesVascular Technology Content OutlineJing CruzPas encore d'évaluation
- Pre Op Hemo ProtocolDocument2 pagesPre Op Hemo ProtocolJing CruzPas encore d'évaluation
- Policies and Statements: Peripheral Arterial UltrasoundDocument5 pagesPolicies and Statements: Peripheral Arterial UltrasoundJing CruzPas encore d'évaluation
- Pre Op Hemo ProtocolDocument2 pagesPre Op Hemo ProtocolJing CruzPas encore d'évaluation
- Implementation Rural AllowancesDocument15 pagesImplementation Rural AllowancesJing CruzPas encore d'évaluation
- Practice Guidelines For Central Venous AccessDocument6 pagesPractice Guidelines For Central Venous AccessJing CruzPas encore d'évaluation
- Clinical Assessment of Ultrasound Equipment Form PDFDocument1 pageClinical Assessment of Ultrasound Equipment Form PDFJing CruzPas encore d'évaluation
- Practice Guidelines For Central Venous Access PDFDocument35 pagesPractice Guidelines For Central Venous Access PDFJulio AltamiranoPas encore d'évaluation
- Ultrasound Technician Resume Example (Saint Mary Hospital OB Clinic) - Wilmington, CaliforniaDocument4 pagesUltrasound Technician Resume Example (Saint Mary Hospital OB Clinic) - Wilmington, CaliforniaJing CruzPas encore d'évaluation
- Ultrasound Technician Resume Example (Grace Medical Clinic) - Quitaque, TexasDocument4 pagesUltrasound Technician Resume Example (Grace Medical Clinic) - Quitaque, TexasJing Cruz0% (1)
- G1 Clinical Application Specialist Resume Example (HITACHI HEALTHCARE AMERICAS) - Cary, IllinoisDocument5 pagesG1 Clinical Application Specialist Resume Example (HITACHI HEALTHCARE AMERICAS) - Cary, IllinoisJing CruzPas encore d'évaluation
- Urs Edu - Hivaids BotswaniaDocument129 pagesUrs Edu - Hivaids BotswaniaJing CruzPas encore d'évaluation
- Point of care ultrasound systems for anesthesia, musculoskeletal and moreDocument4 pagesPoint of care ultrasound systems for anesthesia, musculoskeletal and moreJing CruzPas encore d'évaluation
- HRQ Common Interview QuestionsDocument2 pagesHRQ Common Interview QuestionsJing CruzPas encore d'évaluation
- URS Edu HIVAIDS Window HopeDocument19 pagesURS Edu HIVAIDS Window HopeJing CruzPas encore d'évaluation
- Tools For Evaluating HIV PDFDocument59 pagesTools For Evaluating HIV PDFJing CruzPas encore d'évaluation
- BarryKuebler Lesson1 AssignmentDocument4 pagesBarryKuebler Lesson1 AssignmentBarry KueblerPas encore d'évaluation
- A New Drug-Shelf Arrangement For Reducing MedicatiDocument9 pagesA New Drug-Shelf Arrangement For Reducing MedicatiEmmanuel LawerPas encore d'évaluation
- DAFTAR PUSTAKA SarkomaDocument2 pagesDAFTAR PUSTAKA SarkomaantaniaaaPas encore d'évaluation
- EMTALADocument5 pagesEMTALAJimmy MillerPas encore d'évaluation
- Case Study - MyomaDocument54 pagesCase Study - Myomauvinr100% (1)
- Eyelid Eversion and Inversion Causes and TreatmentsDocument17 pagesEyelid Eversion and Inversion Causes and TreatmentsmanognaaaaPas encore d'évaluation
- CSOM of Middle Ear Part 2Document55 pagesCSOM of Middle Ear Part 2Anindya NandiPas encore d'évaluation
- Multidrug Resistant Gram Negative BacteriaDocument6 pagesMultidrug Resistant Gram Negative BacteriaAniAliciaOrtizCastlePas encore d'évaluation
- Surrogacy AgreementDocument29 pagesSurrogacy AgreementMacduff RonniePas encore d'évaluation
- Ozone Therapy in DentistryDocument16 pagesOzone Therapy in Dentistryshreya das100% (1)
- Amarin V Hikma 331 PDFDocument284 pagesAmarin V Hikma 331 PDFMets FanPas encore d'évaluation
- Balcom Rebecca Functional ResumeDocument2 pagesBalcom Rebecca Functional Resumeapi-360266135Pas encore d'évaluation
- Free Gingival Graft Procedure OverviewDocument1 pageFree Gingival Graft Procedure OverviewTenzin WangyalPas encore d'évaluation
- Healing Stories of People Final EditingDocument53 pagesHealing Stories of People Final Editinggabyk6867% (3)
- Angels Bridging Angels Bridging Angels Bridging Angels Bridging Gaps Gaps Gaps GapsDocument13 pagesAngels Bridging Angels Bridging Angels Bridging Angels Bridging Gaps Gaps Gaps Gapsapi-251664135Pas encore d'évaluation
- Guardian Angel ReikiDocument9 pagesGuardian Angel Reikikoochimetal100% (4)
- 4 Levels of Perio DZDocument2 pages4 Levels of Perio DZKIH 20162017Pas encore d'évaluation
- Vaginitis: Diagnosis and TreatmentDocument9 pagesVaginitis: Diagnosis and TreatmentAbigail MargarethaPas encore d'évaluation
- Types of White Blood CellsDocument2 pagesTypes of White Blood CellsPRINTDESK by DanPas encore d'évaluation
- Genetic Counseling: A Study and SuggestionsDocument10 pagesGenetic Counseling: A Study and SuggestionsraphynjPas encore d'évaluation
- HEX Character Generation Cheat Sheet Version 3Document20 pagesHEX Character Generation Cheat Sheet Version 3NestorDRod100% (1)
- UrinalysisDocument43 pagesUrinalysisJames Knowell75% (4)
- Textbook of Clinical Occupational and Environmental MedicineDocument4 pagesTextbook of Clinical Occupational and Environmental MedicineAmos SiraitPas encore d'évaluation
- Depressive Disorders: PathophysiologyDocument19 pagesDepressive Disorders: Pathophysiology21613284Pas encore d'évaluation
- Maxillofacial Privileges QGHDocument4 pagesMaxillofacial Privileges QGHSanam FaheemPas encore d'évaluation
- BellDocument8 pagesBellZu MiePas encore d'évaluation
- HelmetsDocument13 pagesHelmetsapi-273426812Pas encore d'évaluation
- Chapter Three Research Methodology Study DesignDocument3 pagesChapter Three Research Methodology Study Designotis2ke9588Pas encore d'évaluation
- DylasisDocument3 pagesDylasisyuvi087Pas encore d'évaluation
- Radial Club Hand TreatmentDocument4 pagesRadial Club Hand TreatmentAshu AshPas encore d'évaluation