Vous aimerez peut-être aussi
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocument15 pagesCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoPas encore d'évaluation
- Name: - Year LevelDocument6 pagesName: - Year LevelReda SoPas encore d'évaluation
- Ward Reflection PaperDocument1 pageWard Reflection PaperReda SoPas encore d'évaluation
- Chapter 32 - Genetic Cardiac ArrythmiasDocument7 pagesChapter 32 - Genetic Cardiac ArrythmiasReda SoPas encore d'évaluation
- Chinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Document11 pagesChinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Reda SoPas encore d'évaluation
- Private Ward Admission Census 1Document6 pagesPrivate Ward Admission Census 1Reda SoPas encore d'évaluation
- Answer Key-Mitral ValveDocument6 pagesAnswer Key-Mitral ValveReda SoPas encore d'évaluation
- Trials SummaryDocument12 pagesTrials SummaryReda SoPas encore d'évaluation
- CHAPTER 11: The History and Physical Examination: An Evidence Based ApproachDocument5 pagesCHAPTER 11: The History and Physical Examination: An Evidence Based ApproachReda SoPas encore d'évaluation
- Risk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Document7 pagesRisk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Reda SoPas encore d'évaluation
- Compu Ted Tomogra Phy: (M90Us - LiDocument1 pageCompu Ted Tomogra Phy: (M90Us - LiReda SoPas encore d'évaluation
- EXAM-MITRAL VALVE DISEASE - Reda SoDocument5 pagesEXAM-MITRAL VALVE DISEASE - Reda SoReda SoPas encore d'évaluation
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoPas encore d'évaluation
- Vascular Conference: JUNE 2018 - MARCH 2019Document2 pagesVascular Conference: JUNE 2018 - MARCH 2019Reda SoPas encore d'évaluation
- Rapid Response Team and Cardiac Arrest/Resuscitation TeamDocument11 pagesRapid Response Team and Cardiac Arrest/Resuscitation TeamReda SoPas encore d'évaluation
- ECHO CensusDocument9 pagesECHO CensusReda SoPas encore d'évaluation
- 2011 PadDocument19 pages2011 PadReda SoPas encore d'évaluation
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Document3 pagesCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoPas encore d'évaluation
- Team BLDG LetterDocument1 pageTeam BLDG LetterReda SoPas encore d'évaluation
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoPas encore d'évaluation
- Case Protocol 3Document5 pagesCase Protocol 3Reda SoPas encore d'évaluation
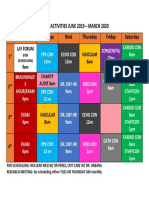
- Daily Activities 2019Document1 pageDaily Activities 2019Reda SoPas encore d'évaluation
- 7 Overview of LipidDocument85 pages7 Overview of LipidReda SoPas encore d'évaluation
- Mckee 2012Document10 pagesMckee 2012Reda SoPas encore d'évaluation
- December 12Document12 pagesDecember 12Reda SoPas encore d'évaluation
- Research ProtocolDocument13 pagesResearch ProtocolReda SoPas encore d'évaluation
- IungDocument8 pagesIungReda SoPas encore d'évaluation
- Sept 3 2017Document7 pagesSept 3 2017Reda SoPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Laporan Puskesmas Kaliasin Feb 2021Document38 pagesLaporan Puskesmas Kaliasin Feb 2021anaz caepPas encore d'évaluation
- Altered Sensorium Batch 2016Document9 pagesAltered Sensorium Batch 2016Adriel PagariganPas encore d'évaluation
- Dry Citrasate Part A Acid Concentrate PowderDocument4 pagesDry Citrasate Part A Acid Concentrate PowderSubhrajit ChattopadhayayPas encore d'évaluation
- PMDC Full Information PaperDocument9 pagesPMDC Full Information PaperjazzyPas encore d'évaluation
- The Effect of 3.2% and 3.8% Sodium CitrateDocument6 pagesThe Effect of 3.2% and 3.8% Sodium CitrateBambang KurniawanPas encore d'évaluation
- ESSAYDocument2 pagesESSAYBokPas encore d'évaluation
- Blood Cells LabDocument7 pagesBlood Cells LabKameron WardPas encore d'évaluation
- Benefits of The Costoclavicular Space For.15Document2 pagesBenefits of The Costoclavicular Space For.15andrew herringPas encore d'évaluation
- Examination of The Gastrointestinal TractDocument44 pagesExamination of The Gastrointestinal TractDrNaveen Singh Rajpurohit Kadu100% (1)
- Good Evening: Ghanta - Chaitanya Iii Year Post Graduate ST - Joseph Dental College Eluru - Andhra PradeshDocument18 pagesGood Evening: Ghanta - Chaitanya Iii Year Post Graduate ST - Joseph Dental College Eluru - Andhra Pradeshchris7982Pas encore d'évaluation
- Ganglion CystDocument3 pagesGanglion CystJuko FernandezPas encore d'évaluation
- 9c5ff54e-92aa-4393-8350-218e91c128d2Document6 pages9c5ff54e-92aa-4393-8350-218e91c128d2Zarbakht AliPas encore d'évaluation
- Fasciolopsis Buski Echinostoma Ilocanum Heterophyes Heterophyes Metagonimus Yokogawai Haplorchis YokogawaiDocument26 pagesFasciolopsis Buski Echinostoma Ilocanum Heterophyes Heterophyes Metagonimus Yokogawai Haplorchis YokogawaiDeepbluexPas encore d'évaluation
- Respiratory MCQs LJDocument7 pagesRespiratory MCQs LJfjghPas encore d'évaluation
- The Critical-Care Pain Observation Tool (CPOT) : Indicator Score DescriptionDocument6 pagesThe Critical-Care Pain Observation Tool (CPOT) : Indicator Score DescriptioncignalPas encore d'évaluation
- Factors Influencing Compliance To Dietary Regimen Among Diabetic Patient in Ladoke Akintola University of Technology Teaching Hospital Osogbo. by Folaranmi Basirat TemitopeDocument98 pagesFactors Influencing Compliance To Dietary Regimen Among Diabetic Patient in Ladoke Akintola University of Technology Teaching Hospital Osogbo. by Folaranmi Basirat TemitopeOMOLOLA ADAMS OLATAYOPas encore d'évaluation
- A. BackgroundDocument17 pagesA. BackgroundErris Tri PrayogoPas encore d'évaluation
- Peritoneal DialysisDocument56 pagesPeritoneal DialysisVanet100% (1)
- MEDL499 - Medical Lab Internship Program - Guidelines - Fall 2022Document31 pagesMEDL499 - Medical Lab Internship Program - Guidelines - Fall 2022Fatima Al IssaPas encore d'évaluation
- Grade 6: The Heart and Circulatory SystemDocument18 pagesGrade 6: The Heart and Circulatory SystemEstanislao Villanueva ElemPas encore d'évaluation
- Case Proforma Final, SurgeryDocument37 pagesCase Proforma Final, SurgeryDiwakesh C B100% (4)
- Drug Study - HydrocortisoneDocument5 pagesDrug Study - HydrocortisoneryanPas encore d'évaluation
- Reading - Age With Moderate DehydrationDocument8 pagesReading - Age With Moderate DehydrationSophia IbuyanPas encore d'évaluation
- BBJJJDocument96 pagesBBJJJBogdan ȘtefîrcăPas encore d'évaluation
- Renal Function TestsDocument23 pagesRenal Function TestsKer YehunPas encore d'évaluation
- Presentation DH (Repaired)Document22 pagesPresentation DH (Repaired)Anmol SinghPas encore d'évaluation
- India's 1 Health Management LabDocument14 pagesIndia's 1 Health Management LabAjay Kumar dasPas encore d'évaluation
- Health Effects of Smoking Among Young PeopleDocument2 pagesHealth Effects of Smoking Among Young PeopleJessicaPas encore d'évaluation
- Muscular System FunctionDocument2 pagesMuscular System FunctionLachlan PalmerPas encore d'évaluation
- Shen Ling Bai Zhu San - 參苓白術散 - Ginseng, Poria and Atractylodis Macrocephalae Powder - 參苓白術散 - Ginseng and Atractylodes Formula - Chinese Herbs - American Dragon - Dr Joel Penner OMD, LAcDocument9 pagesShen Ling Bai Zhu San - 參苓白術散 - Ginseng, Poria and Atractylodis Macrocephalae Powder - 參苓白術散 - Ginseng and Atractylodes Formula - Chinese Herbs - American Dragon - Dr Joel Penner OMD, LAcangelesarenas0% (1)