Vous aimerez peut-être aussi
- Case ReportDocument57 pagesCase ReportlmandahaPas encore d'évaluation
- Tibia ProximalDocument51 pagesTibia Proximalchenth3r3Pas encore d'évaluation
- Fracture Tibia & Fibula-1Document111 pagesFracture Tibia & Fibula-1Usaid SulaimanPas encore d'évaluation
- Scapula Fracture Treatment & Management: Author: Thomas P Goss, MD Chief Editor: S Ashfaq Hasan, MDDocument24 pagesScapula Fracture Treatment & Management: Author: Thomas P Goss, MD Chief Editor: S Ashfaq Hasan, MDjohanesPas encore d'évaluation
- Femoral Supracondylar Fractures: Prepared by Dr. Ramzy Sh. ShikhanDocument77 pagesFemoral Supracondylar Fractures: Prepared by Dr. Ramzy Sh. ShikhanRamzi ShukriPas encore d'évaluation
- Conservative Treatment of Diaphyseal Fractures of Tibia andDocument40 pagesConservative Treatment of Diaphyseal Fractures of Tibia andsaihaPas encore d'évaluation
- Lect 8 Lower Extremity Fracture 2Document22 pagesLect 8 Lower Extremity Fracture 220-221 Crisny Novika Yely Br. HutagaolPas encore d'évaluation
- Fracture Shaft Humerus - 030014Document60 pagesFracture Shaft Humerus - 030014MohammedShahidPas encore d'évaluation
- Fractures of The Humeral ShaftDocument25 pagesFractures of The Humeral ShaftMuhammad IqbalPas encore d'évaluation
- Fractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyasDocument90 pagesFractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyaspattiyahPas encore d'évaluation
- ORP - Handout - English - Malleolar FracturesDocument15 pagesORP - Handout - English - Malleolar Fracturesadrian1989Pas encore d'évaluation
- Musculoskeletal Trauma Cases in Lower Extremities and Its ManagementDocument41 pagesMusculoskeletal Trauma Cases in Lower Extremities and Its ManagementAli AbdullahPas encore d'évaluation
- Femoral Fracture: Fathiyah BT Mazlan 4 Year Medical Student Quest International University of PerakDocument28 pagesFemoral Fracture: Fathiyah BT Mazlan 4 Year Medical Student Quest International University of PerakNinaPas encore d'évaluation
- Knee Tibia & Ankle InjuriesDocument88 pagesKnee Tibia & Ankle InjuriesNasser AlQadhibPas encore d'évaluation
- Forearm Fracture 1 BismillahDocument17 pagesForearm Fracture 1 Bismillahamel015Pas encore d'évaluation
- Nursing Management: Musculoskeletal Trauma and Orthopedic SurgeryDocument25 pagesNursing Management: Musculoskeletal Trauma and Orthopedic SurgeryDeannahTampusPas encore d'évaluation
- Lecture 7 Femoral Diapisis and Distal FDocument16 pagesLecture 7 Femoral Diapisis and Distal FQueen SofiaPas encore d'évaluation
- Case Study of "Subtrochanteric Femur": Prepared By: John Ress A. Escobal Group 1Document11 pagesCase Study of "Subtrochanteric Femur": Prepared By: John Ress A. Escobal Group 1J.r. MercadoPas encore d'évaluation
- Clavicle Fracture, SC Joint and Ac Joint Injury: Team IiiDocument19 pagesClavicle Fracture, SC Joint and Ac Joint Injury: Team IiiJunarto Putra TandiarrangPas encore d'évaluation
- Hip FracturesDocument74 pagesHip FracturesMina SamirPas encore d'évaluation
- U04 Fxs of Humeral ShaftDocument88 pagesU04 Fxs of Humeral Shaftadrian_mogosPas encore d'évaluation
- Scapula FracturesDocument24 pagesScapula FracturesFrancesco BenazzoPas encore d'évaluation
- Injury Around The Elbow: Mohamad Afiq Izzuddin 1001336000 Group 3Document51 pagesInjury Around The Elbow: Mohamad Afiq Izzuddin 1001336000 Group 3Star CruisePas encore d'évaluation
- Elbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsDocument57 pagesElbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsHajar AlSaediPas encore d'évaluation
- Principles of ImmobilizationDocument27 pagesPrinciples of ImmobilizationSivaneasan KandiahPas encore d'évaluation
- Mallet FingerDocument14 pagesMallet FingerMuskan MuhemmedPas encore d'évaluation
- 4 150512145223 Lva1 App6891Document40 pages4 150512145223 Lva1 App6891Rizky HandayaniPas encore d'évaluation
- Pilon FractureDocument49 pagesPilon FractureJinnasit TeePas encore d'évaluation
- Ender Nailing in HumerusDocument56 pagesEnder Nailing in HumerusRakesh KumarPas encore d'évaluation
- OPEN FRACTURES Final Dr. Nishith SharmaDocument41 pagesOPEN FRACTURES Final Dr. Nishith SharmaNishith SharmaPas encore d'évaluation
- Coronoid FractureDocument38 pagesCoronoid FractureRamin MaharjanPas encore d'évaluation
- 6-Fractures and Joints Dislocations ManagementDocument91 pages6-Fractures and Joints Dislocations ManagementMUGISHA GratienPas encore d'évaluation
- Fractures HFHDocument74 pagesFractures HFHEmmanuel Papa AcquahPas encore d'évaluation
- Injuries Around The ShoulderDocument81 pagesInjuries Around The ShoulderMisoPas encore d'évaluation
- LowerDocument89 pagesLowerBedo GikryPas encore d'évaluation
- Paediatric FracturesDocument23 pagesPaediatric Fracturesjerry999Pas encore d'évaluation
- Humeral Shaft FractureDocument82 pagesHumeral Shaft FractureYoga AninditaPas encore d'évaluation
- Fracture Dan Penanganan EmergencyDocument52 pagesFracture Dan Penanganan Emergencyshindie lethulurPas encore d'évaluation
- Proximal Humeral Fracture Repair and RehabilitationDocument8 pagesProximal Humeral Fracture Repair and RehabilitationAnonymous UClts4nYPas encore d'évaluation
- Tibial PlateauDocument43 pagesTibial Plateauamal.fathullahPas encore d'évaluation
- Ortho PresentationDocument21 pagesOrtho PresentationAkmal ZaibPas encore d'évaluation
- Arthroplasty of Shoulder - MKKPPTXDocument54 pagesArthroplasty of Shoulder - MKKPPTXMis StromPas encore d'évaluation
- Common Lower Limb Fracture: DR Tarif Alakhras Orthopedic Surgeon KFMCDocument49 pagesCommon Lower Limb Fracture: DR Tarif Alakhras Orthopedic Surgeon KFMCahmad albab100% (1)
- Fracture: Suchithra.P.V 1 Year Msc. Nursing College of Nursing AlappuzhaDocument96 pagesFracture: Suchithra.P.V 1 Year Msc. Nursing College of Nursing AlappuzhaAakash A. AgrawalPas encore d'évaluation
- Distal Radial Injury: Department of Orthopaedics SGH Didactic LectureDocument52 pagesDistal Radial Injury: Department of Orthopaedics SGH Didactic Lecturedrscribd1Pas encore d'évaluation
- 2.supracondylar Humerus FracturesDocument26 pages2.supracondylar Humerus FracturesDabessa MosissaPas encore d'évaluation
- Seminar On Upper Limb FractureDocument166 pagesSeminar On Upper Limb FractureArko dutta100% (1)
- Blue Writing Is What I Added To These Notes: RadiographyDocument46 pagesBlue Writing Is What I Added To These Notes: Radiographybjpalmer100% (2)
- Patellar Fracture 1Document39 pagesPatellar Fracture 1Syafiq ShahbudinPas encore d'évaluation
- Lower Extremity Bone Fracture Lecture 3Document88 pagesLower Extremity Bone Fracture Lecture 3Tselmeg TselmegPas encore d'évaluation
- Lower Limb FracturesDocument124 pagesLower Limb Fracturesmau tau100% (1)
- 7 Injuries of Upper Arm and ElbowDocument75 pages7 Injuries of Upper Arm and Elbowwissam salimPas encore d'évaluation
- LisfrancDocument25 pagesLisfrancSamir AsmarPas encore d'évaluation
- Fractures of Shoulder and Elbow EditedDocument25 pagesFractures of Shoulder and Elbow EditedSurgicalgownPas encore d'évaluation
- Malleolar Fractures - Handout PDFDocument14 pagesMalleolar Fractures - Handout PDFAlin Bratu100% (2)
- Lower Limb Fracture..MeDocument142 pagesLower Limb Fracture..MeWorku KiflePas encore d'évaluation
- Clavicle FractureDocument33 pagesClavicle FractureNitin AggarwalPas encore d'évaluation
- Immobilization and Transport On Patient FractureDocument58 pagesImmobilization and Transport On Patient FractureDinaPas encore d'évaluation
- Patellar FractureDocument25 pagesPatellar FractureSyafiq ShahbudinPas encore d'évaluation
- Reduction, Relocation and Splinting in Emergency Room (RASER)D'EverandReduction, Relocation and Splinting in Emergency Room (RASER)Pas encore d'évaluation
- Esophageal Perforation TreatmentDocument4 pagesEsophageal Perforation TreatmentDabessa MosissaPas encore d'évaluation
- Management of Hepatic CystsDocument12 pagesManagement of Hepatic CystsDabessa MosissaPas encore d'évaluation
- Whipple ProcedureDocument16 pagesWhipple ProcedureDabessa MosissaPas encore d'évaluation
- Open Radical Cholecystectomy With Partial Hepatectomy For Gallbladder CancerDocument2 pagesOpen Radical Cholecystectomy With Partial Hepatectomy For Gallbladder CancerDabessa MosissaPas encore d'évaluation
- General Consideration in EsophagectomyDocument4 pagesGeneral Consideration in EsophagectomyDabessa MosissaPas encore d'évaluation
- Techniques of Exposure, Hilar DissectionDocument20 pagesTechniques of Exposure, Hilar DissectionDabessa MosissaPas encore d'évaluation
- Flexor Tendon AnatomyDocument29 pagesFlexor Tendon AnatomyDabessa MosissaPas encore d'évaluation
- 2.supracondylar Humerus FracturesDocument26 pages2.supracondylar Humerus FracturesDabessa MosissaPas encore d'évaluation
- Common FractureDocument314 pagesCommon FractureDabessa MosissaPas encore d'évaluation
- External FixatorDocument19 pagesExternal FixatorDabessa MosissaPas encore d'évaluation
- Fractures of The Femoral NeckDocument37 pagesFractures of The Femoral NeckDabessa MosissaPas encore d'évaluation
- Congenital Diaphragmatic HerniaDocument45 pagesCongenital Diaphragmatic HerniaDabessa MosissaPas encore d'évaluation
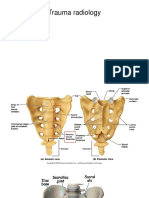
- Trauma RadiologyDocument9 pagesTrauma RadiologyDabessa MosissaPas encore d'évaluation
- Hand IncisionsDocument55 pagesHand IncisionsDabessa Mosissa100% (2)
- Midfoot TraumaDocument26 pagesMidfoot TraumaDabessa MosissaPas encore d'évaluation
- Trauma RadiologyDocument9 pagesTrauma RadiologyDabessa MosissaPas encore d'évaluation
- Soft Tissue TumorDocument248 pagesSoft Tissue TumorDabessa MosissaPas encore d'évaluation
- Fingertip AmputationDocument41 pagesFingertip AmputationDabessa MosissaPas encore d'évaluation
- Surgical Approaches and Applied AnatomyDocument44 pagesSurgical Approaches and Applied AnatomyDabessa MosissaPas encore d'évaluation
- Humerous Fxs With Radial Nerve PalsyDocument26 pagesHumerous Fxs With Radial Nerve PalsyDabessa MosissaPas encore d'évaluation
- Trigger Finger (TF)Document59 pagesTrigger Finger (TF)Dabessa MosissaPas encore d'évaluation
- The ForearmDocument49 pagesThe ForearmDabessa MosissaPas encore d'évaluation
- The ForearmDocument49 pagesThe ForearmDabessa MosissaPas encore d'évaluation
- Bone and Joint InfectionsDocument153 pagesBone and Joint InfectionsDabessa MosissaPas encore d'évaluation
- EsophagusDocument24 pagesEsophagusDabessa MosissaPas encore d'évaluation
- JaundiceDocument12 pagesJaundiceDabessa MosissaPas encore d'évaluation
- Pediatric Surgical ThemesDocument32 pagesPediatric Surgical ThemesDabessa MosissaPas encore d'évaluation
- Discribd DocumentDocument1 pageDiscribd DocumentDabessa MosissaPas encore d'évaluation
- Discribd DocumentDocument1 pageDiscribd DocumentDabessa MosissaPas encore d'évaluation
- Extremity TraumaDocument31 pagesExtremity TraumaPap Pip100% (1)
- PE9 - q1 - Melc1 - FIRST AIDDocument16 pagesPE9 - q1 - Melc1 - FIRST AIDRojegarmil LagoPas encore d'évaluation
- Accident EnrollKit - CVS HealthDocument19 pagesAccident EnrollKit - CVS Healthvashista.guzmanPas encore d'évaluation
- Christopher H. Wise - Mobilization Notes - A Rehabilitation Specialist's Pocket GuideDocument240 pagesChristopher H. Wise - Mobilization Notes - A Rehabilitation Specialist's Pocket GuideRukaphuongPas encore d'évaluation
- Fracture and Joint Injuries (Shalter-Chapter 15) - Kelompok C (Dr. Oktavianus, SP - Ot)Document69 pagesFracture and Joint Injuries (Shalter-Chapter 15) - Kelompok C (Dr. Oktavianus, SP - Ot)Heru ChrisPas encore d'évaluation
- Practice in South India: Puttur Kattu (Bandage) - A Traditional Bone SettingDocument5 pagesPractice in South India: Puttur Kattu (Bandage) - A Traditional Bone SettingbahbaguruPas encore d'évaluation
- A Manual of Orthopaedic Terminology PDFDocument508 pagesA Manual of Orthopaedic Terminology PDFVasiPas encore d'évaluation
- Artikel 5 Siap TerbitDocument11 pagesArtikel 5 Siap Terbithobi kitaPas encore d'évaluation
- UNIT 5 Explanation TextDocument18 pagesUNIT 5 Explanation TextFardika ArmawantoPas encore d'évaluation
- Musculoskeletal DisordersDocument8 pagesMusculoskeletal DisordersShaina Joy SaballoPas encore d'évaluation
- P.7 Sci Lesson NotesDocument61 pagesP.7 Sci Lesson NotesAlex SsembalirwaPas encore d'évaluation
- Trauma CompleteDocument128 pagesTrauma Completeashvin_7Pas encore d'évaluation
- Ankle Dislocations Health Conference 2010Document16 pagesAnkle Dislocations Health Conference 2010Aswan IsmailPas encore d'évaluation
- Health Ed II Module 5Document15 pagesHealth Ed II Module 5saturnino corpuzPas encore d'évaluation
- Complete Ortho PDFDocument204 pagesComplete Ortho PDFLorraineYong100% (4)
- HOPE 1st Quarter ExamDocument4 pagesHOPE 1st Quarter ExamWiljhon Espinola Julapong100% (1)
- Musculoskeleteal ReviewerDocument24 pagesMusculoskeleteal ReviewerRobert BoongalingPas encore d'évaluation
- Grade 9 1st QuarterDocument5 pagesGrade 9 1st QuarterRenlieLegaspiPas encore d'évaluation
- Muskuloskeletal DisordersDocument15 pagesMuskuloskeletal DisordersLienyPerasPas encore d'évaluation
- Things To Read: A. Trauma: Fractures and DislocationsDocument4 pagesThings To Read: A. Trauma: Fractures and DislocationsHanien YeePas encore d'évaluation
- Fix Me I'm Broken (On First Aid)Document21 pagesFix Me I'm Broken (On First Aid)Romar LagunaPas encore d'évaluation
- SJA First Aid Club Lesson Plan Bones Muscles and Joints Resource PDFDocument2 pagesSJA First Aid Club Lesson Plan Bones Muscles and Joints Resource PDFjanreyPas encore d'évaluation
- Dance Relate InjuriesDocument54 pagesDance Relate InjuriesApryll Anne Edades100% (1)
- Basilar Invagination - C1-C2 DistractionDocument6 pagesBasilar Invagination - C1-C2 DistractionSri Vijay Anand K SPas encore d'évaluation
- Acromioclavicular InjuriesDocument11 pagesAcromioclavicular Injurieslou_gehrig2001Pas encore d'évaluation
- 4-09 Trauma - Musculoskeletal TraumaDocument18 pages4-09 Trauma - Musculoskeletal TraumaEmil CotenescuPas encore d'évaluation
- PE11 Q4 Module4a Weeks1and2Document19 pagesPE11 Q4 Module4a Weeks1and2Ariel PagoboPas encore d'évaluation
- Instructions On How To Properly Fill in The WAIRDocument17 pagesInstructions On How To Properly Fill in The WAIRLauro CanceranPas encore d'évaluation
- 3rd Periodical Test GRADE 11Document1 page3rd Periodical Test GRADE 11Jessieann Balmaceda Cabangan100% (3)
- Done-EDITED-HOPE1 q1 Mod5 ObservesPersonalSafetyProtocol-1Document18 pagesDone-EDITED-HOPE1 q1 Mod5 ObservesPersonalSafetyProtocol-1Mary Gloriscislle M. JorePas encore d'évaluation