Vous aimerez peut-être aussi
- Mci, Dementia, Alzheimer DiseaseDocument60 pagesMci, Dementia, Alzheimer DiseaseDave Siahaan de KaratekaPas encore d'évaluation
- DementiaDocument12 pagesDementiaPriscila SelingardiPas encore d'évaluation
- Surgical Pathology - Diseases of The Central Nervous System 401 - Dr. Baby Lynne Asuncion - October 20-28, 2014Document10 pagesSurgical Pathology - Diseases of The Central Nervous System 401 - Dr. Baby Lynne Asuncion - October 20-28, 2014atb_phPas encore d'évaluation
- "Clinical Study of Memory Disorders in Aging Patients With Associated Cardiovascular, Neurological, Neurobehavioral and Metabolic Diseases". A ReviewDocument9 pages"Clinical Study of Memory Disorders in Aging Patients With Associated Cardiovascular, Neurological, Neurobehavioral and Metabolic Diseases". A ReviewSketchy PathPas encore d'évaluation
- Dementia Dementia Is Marked by Severe Impairment in Memory, Judgment, Orientation, and CognitionDocument9 pagesDementia Dementia Is Marked by Severe Impairment in Memory, Judgment, Orientation, and CognitionAkhmad Ulil AlbabPas encore d'évaluation
- Pediatric StrokeDocument43 pagesPediatric StrokePrachiti KarodePas encore d'évaluation
- Vascular DementiaDocument57 pagesVascular Dementiadrkadiyala2100% (3)
- Stroke and Dementia: Dr. Dr. Suherman, SP.S (K)Document36 pagesStroke and Dementia: Dr. Dr. Suherman, SP.S (K)deri rivanoPas encore d'évaluation
- Vascular DementiaDocument57 pagesVascular Dementiadrkadiyala2Pas encore d'évaluation
- 42.0 Demyelinating and Degenerative Diseases of CNS 2022 PDFDocument66 pages42.0 Demyelinating and Degenerative Diseases of CNS 2022 PDFhuda dotPas encore d'évaluation
- Dementia AssignmentDocument19 pagesDementia AssignmentVandna Vikram Novlani50% (2)
- CVA Case Study 3BDocument20 pagesCVA Case Study 3BLord Allen B. GomezPas encore d'évaluation
- Index - : Professor Yasser MetwallyDocument11 pagesIndex - : Professor Yasser MetwallyDrhikmatullah SheraniPas encore d'évaluation
- Cognition, Mood and Behavior in CADASILDocument6 pagesCognition, Mood and Behavior in CADASILAna Carolina RibasPas encore d'évaluation
- Neurological Manifestations of Vascular DementiaDocument5 pagesNeurological Manifestations of Vascular DementiaDumitruAuraPas encore d'évaluation
- Javad Jamshidi MSC of Human Geneticas Shahid Beheshti University of Medical Sciences J.Jamshidi@Sbmu - Ac.IrDocument21 pagesJavad Jamshidi MSC of Human Geneticas Shahid Beheshti University of Medical Sciences J.Jamshidi@Sbmu - Ac.IrabolojeenPas encore d'évaluation
- CH 23 - Nervous System PDFDocument2 pagesCH 23 - Nervous System PDFKgerbPas encore d'évaluation
- DementiaDocument60 pagesDementiaRuaa HdeibPas encore d'évaluation
- Sample DementiaDocument5 pagesSample DementiaAlina LazărPas encore d'évaluation
- Stroke Syndromes and Localization 2007Document56 pagesStroke Syndromes and Localization 2007SaintPaul Univ100% (1)
- Assessment Task-3 (Dementia Disease)Document10 pagesAssessment Task-3 (Dementia Disease)Ashesh BasnetPas encore d'évaluation
- Cerebral Amyloid Angiopathy-Medscape (2023 - 10 - 28)Document11 pagesCerebral Amyloid Angiopathy-Medscape (2023 - 10 - 28)Apostolos T.Pas encore d'évaluation
- Deg ModuleDocument15 pagesDeg Modulebiswajitpaul8403Pas encore d'évaluation
- Dementia: Dementia, Also Referred To As Major Neurocognitive Disorder in DSM-5, IsDocument20 pagesDementia: Dementia, Also Referred To As Major Neurocognitive Disorder in DSM-5, IsTurky DallolPas encore d'évaluation
- Ataxia and Movement Disorders: Clinical Manifestations TreatmentDocument6 pagesAtaxia and Movement Disorders: Clinical Manifestations TreatmentMahfouzPas encore d'évaluation
- Emerging Molecular Mechanisms of Vascular Dementia: ReviewDocument8 pagesEmerging Molecular Mechanisms of Vascular Dementia: ReviewJuan Jose Eraso OsorioPas encore d'évaluation
- Cerebrovascular Diseas1Document47 pagesCerebrovascular Diseas1Jenard Joniel OlivarPas encore d'évaluation
- Final Stroke MBDocument79 pagesFinal Stroke MBVanessa Yvonne GurtizaPas encore d'évaluation
- Alzheimer FinalDocument121 pagesAlzheimer FinalJoanne Foja100% (1)
- Med Surg A Neuro PPT 120515134413541 5Document93 pagesMed Surg A Neuro PPT 120515134413541 5Sapiah RamanPas encore d'évaluation
- Vascular Dementia: Prevention and Treatment: Catherine Mcveigh Peter PassmoreDocument7 pagesVascular Dementia: Prevention and Treatment: Catherine Mcveigh Peter PassmoreShelia LewisPas encore d'évaluation
- Vascular DementiaDocument8 pagesVascular Dementiaddelindaaa100% (1)
- Neurocognitive Disorders: Masumura Miraato PascoDocument27 pagesNeurocognitive Disorders: Masumura Miraato PascoportiadeportiaPas encore d'évaluation
- Etiology of DementiaDocument7 pagesEtiology of DementiaAirene SiblePas encore d'évaluation
- Practice EssentialsDocument18 pagesPractice EssentialsKusno TriantoPas encore d'évaluation
- Conners2011 PDFDocument297 pagesConners2011 PDFCristinaPas encore d'évaluation
- Dementia and How The Dementic Patients' Are?Document50 pagesDementia and How The Dementic Patients' Are?Faria Islam JuhiPas encore d'évaluation
- Fnagi 05 00017Document19 pagesFnagi 05 00017mariamojegPas encore d'évaluation
- DEMENTIA - Neurological DisordersDocument12 pagesDEMENTIA - Neurological DisorderspreveennaPas encore d'évaluation
- Failing: Dementia: The BrainDocument4 pagesFailing: Dementia: The BrainAleja ToPaPas encore d'évaluation
- Nar SingDocument14 pagesNar Singbasinang_jangilPas encore d'évaluation
- Pemicu 6 Sarafff (Autosaved)Document20 pagesPemicu 6 Sarafff (Autosaved)cecilliacynthiaPas encore d'évaluation
- J Emc 2016 06 017 PDFDocument17 pagesJ Emc 2016 06 017 PDFnonniPas encore d'évaluation
- DementiaDocument38 pagesDementiarajikakurupPas encore d'évaluation
- CNS IDocument6 pagesCNS IYixin XuPas encore d'évaluation
- Neuropatologia AlzheimerDocument27 pagesNeuropatologia AlzheimerSarah JatobáPas encore d'évaluation
- Cadasil Syndrome: A Case Report With A Literature ReviewDocument4 pagesCadasil Syndrome: A Case Report With A Literature ReviewAna Carolina RibasPas encore d'évaluation
- Lecture 16 - DementiaDocument44 pagesLecture 16 - Dementiaepic sound everPas encore d'évaluation
- Disease of Nervous System Lect 2Document62 pagesDisease of Nervous System Lect 2Monirul IslamPas encore d'évaluation
- Chapter 14 Cognitive DisordersDocument43 pagesChapter 14 Cognitive DisordersClaire Go TajarrosPas encore d'évaluation
- Alzheimer Disease and Other DementiasDocument28 pagesAlzheimer Disease and Other DementiasIlham 123456Pas encore d'évaluation
- Review Article: George P. Paraskevas, Vasilios C. Constantinides, Panagiotis G. Paraskevas, Elisabeth KapakiDocument6 pagesReview Article: George P. Paraskevas, Vasilios C. Constantinides, Panagiotis G. Paraskevas, Elisabeth KapakiasclepiuspdfsPas encore d'évaluation
- Differential Diagnosis and StrokeDocument38 pagesDifferential Diagnosis and StrokeAin AmanyPas encore d'évaluation
- Vascular DementiaDocument7 pagesVascular DementiaAAshish singh BhadoriyaPas encore d'évaluation
- Dementia 2005Document46 pagesDementia 2005sankethPas encore d'évaluation
- Myelination in Pediatric NeurologyDocument41 pagesMyelination in Pediatric NeurologyAna Bărdaș-ZugravuPas encore d'évaluation
- Refrat Vascular DementiaDocument12 pagesRefrat Vascular DementiaDebri ErwendiPas encore d'évaluation
- StrokeDocument102 pagesStrokea20-0353-958Pas encore d'évaluation
- Middle Cerebral Artery (MCA) Infarction: Jenis Stroke IskemikDocument7 pagesMiddle Cerebral Artery (MCA) Infarction: Jenis Stroke IskemiksarelriskyPas encore d'évaluation
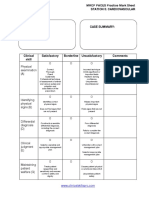
- Station 3 Neurology MRCP PACES Mark SheetDocument1 pageStation 3 Neurology MRCP PACES Mark SheetdoctorebrahimPas encore d'évaluation
- Station 2 History MRCP PACES Practice Mark SheetDocument1 pageStation 2 History MRCP PACES Practice Mark SheetdoctorebrahimPas encore d'évaluation
- In DiabetesDocument1 pageIn DiabetesdoctorebrahimPas encore d'évaluation
- Station 1 Abdominal MRCP PACES Practice Mark SheetDocument1 pageStation 1 Abdominal MRCP PACES Practice Mark SheetdoctorebrahimPas encore d'évaluation
- CANOMODDocument9 pagesCANOMODdoctorebrahimPas encore d'évaluation
- Station 3 Cardiovascular MRCP PACES Practice Mark SheetDocument1 pageStation 3 Cardiovascular MRCP PACES Practice Mark SheetdoctorebrahimPas encore d'évaluation
- Carlo Wilke - NFL in SCA1 and MSA CDocument12 pagesCarlo Wilke - NFL in SCA1 and MSA CdoctorebrahimPas encore d'évaluation
- CANOMAD Responding To Weekly IV ImmunoglobulinDocument4 pagesCANOMAD Responding To Weekly IV ImmunoglobulindoctorebrahimPas encore d'évaluation
- Skin Involvement in Atypical Hemolytic Uremic SyndromeDocument4 pagesSkin Involvement in Atypical Hemolytic Uremic SyndromedoctorebrahimPas encore d'évaluation
- Adam Vogel - Challenges and Possibilities of Automated Speech Monitoring in AtaxiaDocument15 pagesAdam Vogel - Challenges and Possibilities of Automated Speech Monitoring in AtaxiadoctorebrahimPas encore d'évaluation
- Impact of DM On MIDocument13 pagesImpact of DM On MIdoctorebrahimPas encore d'évaluation
- Stroke and Transient Ischaemic Attack in Over 16s Diagnosis and Initial Management PDF 66141665603269Document48 pagesStroke and Transient Ischaemic Attack in Over 16s Diagnosis and Initial Management PDF 66141665603269doctorebrahimPas encore d'évaluation
- The Rare and The Unexpected Miller Fisher SyndromeDocument4 pagesThe Rare and The Unexpected Miller Fisher SyndromedoctorebrahimPas encore d'évaluation
- Variants of Guillainbarre Syndrome Miller Fisher Syndrome Facial Diplegia and Multiple Cranial Nerve PalsiesDocument6 pagesVariants of Guillainbarre Syndrome Miller Fisher Syndrome Facial Diplegia and Multiple Cranial Nerve PalsiesdoctorebrahimPas encore d'évaluation
- Approach To The Patient With Suspected Immunodeficiency - Immunology Allergic Disorders - Merck Manuals Professional EditionDocument15 pagesApproach To The Patient With Suspected Immunodeficiency - Immunology Allergic Disorders - Merck Manuals Professional EditiondoctorebrahimPas encore d'évaluation
- Order #Fo3aa22827c4Document4 pagesOrder #Fo3aa22827c4Solo GathogoPas encore d'évaluation
- Attachment - Relational-Needs - and - Psychotherapeutic - Richard ErskineDocument10 pagesAttachment - Relational-Needs - and - Psychotherapeutic - Richard ErskineЕлена КабрановаPas encore d'évaluation
- Clinical Study On Acupuncture For Quality of Life in Patients With Age-Related Macular DegenerationDocument5 pagesClinical Study On Acupuncture For Quality of Life in Patients With Age-Related Macular DegenerationathiaPas encore d'évaluation
- Peripheral Oedema (Assessment Of) - Diagnosis - Approach - Best Practice - EspañolDocument4 pagesPeripheral Oedema (Assessment Of) - Diagnosis - Approach - Best Practice - EspañolOscar Castro CuaquiraPas encore d'évaluation
- Qingling Haung Resume - HcaDocument4 pagesQingling Haung Resume - Hcaapi-317607382Pas encore d'évaluation
- The Differences Between Coaching Mentoring Therapy and Counselling PDFDocument5 pagesThe Differences Between Coaching Mentoring Therapy and Counselling PDFghinaPas encore d'évaluation
- Grievance Status RMLDocument1 pageGrievance Status RMLMayankPas encore d'évaluation
- Arora 2009Document6 pagesArora 2009ece142Pas encore d'évaluation
- Vitamins: (DR Pauling Recommendation, Svaki Dan Uzeti)Document3 pagesVitamins: (DR Pauling Recommendation, Svaki Dan Uzeti)Veky VictoriaPas encore d'évaluation
- Exemestane Aromasin InsertDocument4 pagesExemestane Aromasin InsertKane SmithPas encore d'évaluation
- HSDC QuintesenceDocument6 pagesHSDC QuintesenceDavid CasaverdePas encore d'évaluation
- Simple Guide Orthopadics Chapter 11 Neurological and Spinal ConditionsDocument86 pagesSimple Guide Orthopadics Chapter 11 Neurological and Spinal ConditionsSurgicalgownPas encore d'évaluation
- Medication Calculation Practice Problems: Level Ii, Iii and IvDocument6 pagesMedication Calculation Practice Problems: Level Ii, Iii and IvQueennita100% (7)
- Gender Identity DisorderDocument21 pagesGender Identity Disorderlshapiro8869Pas encore d'évaluation
- NPD Elsa RonningstamDocument15 pagesNPD Elsa RonningstamFrancescaPas encore d'évaluation
- Gateway B2 Test 6A 1-3 PDFDocument3 pagesGateway B2 Test 6A 1-3 PDFlourdes100% (1)
- NCLEX Questions 96-105Document3 pagesNCLEX Questions 96-105kxviperPas encore d'évaluation
- Nurse Deployment Program Journal FebruaryDocument3 pagesNurse Deployment Program Journal FebruaryMenchie Vivas-Alot100% (1)
- Pathology QuestionsDocument67 pagesPathology QuestionsRedentor MagdayaoPas encore d'évaluation
- Ikg05 Sap Preparasi Saluran AkarDocument54 pagesIkg05 Sap Preparasi Saluran AkarSyifa Syafitri100% (1)
- Traumatic Intracerebral Hemorrhage: Risk Factors Associated With ProgressionDocument35 pagesTraumatic Intracerebral Hemorrhage: Risk Factors Associated With ProgressionPavel SebastianPas encore d'évaluation
- Hemangioma PresentationDocument18 pagesHemangioma Presentationplastic guardiansPas encore d'évaluation
- Pseudomonarchia DaemonumDocument7 pagesPseudomonarchia DaemonumManuel AlorPas encore d'évaluation
- Frank Ros The Lost Secrets of Ayurvedic AcupunctureDocument228 pagesFrank Ros The Lost Secrets of Ayurvedic AcupuncturePrasana Siva100% (6)
- Virtual Reality One-Session Treatment of Child-Specific Phobia of Dogs: A Controlled, Multiple Baseline Case SeriesDocument14 pagesVirtual Reality One-Session Treatment of Child-Specific Phobia of Dogs: A Controlled, Multiple Baseline Case SeriesOscar Luis Ballesta ChPas encore d'évaluation
- Fibromyalgia: Points To Remember About FibromyalgiaDocument6 pagesFibromyalgia: Points To Remember About FibromyalgiaeliseeaPas encore d'évaluation
- Topnotch Integrative MedicineDocument65 pagesTopnotch Integrative Medicinemefav7778520Pas encore d'évaluation
- Investigating The Factors Influencing Professional Identity of First Year Health and Social Care Students PDFDocument14 pagesInvestigating The Factors Influencing Professional Identity of First Year Health and Social Care Students PDFMariana CiceuPas encore d'évaluation
- Hipertension in Pregnancy - QuestionDocument3 pagesHipertension in Pregnancy - QuestionkoassspkkPas encore d'évaluation
- Nle Tips MS PDFDocument11 pagesNle Tips MS PDFjthsPas encore d'évaluation