Vous aimerez peut-être aussi
- Central Nervous System Depressant Drug Abuse And Addiction:: Implications for CounselingD'EverandCentral Nervous System Depressant Drug Abuse And Addiction:: Implications for CounselingPas encore d'évaluation
- ECT CompDocument23 pagesECT CompPinak DePas encore d'évaluation
- ECT ManualDocument57 pagesECT ManualyeivierPas encore d'évaluation
- Psychiatric Diagnosis: Challenges and ProspectsD'EverandPsychiatric Diagnosis: Challenges and ProspectsIhsan M. SalloumÉvaluation : 5 sur 5 étoiles5/5 (1)
- Somatics Brochure Thymatron PDFDocument8 pagesSomatics Brochure Thymatron PDFCumhur TaşPas encore d'évaluation
- Basic PsychiatryDocument338 pagesBasic PsychiatryAlison ChangPas encore d'évaluation
- Electroconvulsive Therapy: An UpdateDocument39 pagesElectroconvulsive Therapy: An UpdateAnonymous 83o62cPas encore d'évaluation
- Pain PathwaysDocument45 pagesPain PathwaysKabirPas encore d'évaluation
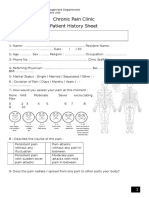
- Chronic Pain Clinic Patient History SheetDocument4 pagesChronic Pain Clinic Patient History SheetBelal N. MahfouzPas encore d'évaluation
- MHA Ect GuidelinesDocument151 pagesMHA Ect GuidelinesDian AfrisiaPas encore d'évaluation
- ECT Dosing ParametersDocument2 pagesECT Dosing ParametersdocmojoPas encore d'évaluation
- Medical Emergencies in Rehabilitation MedicineDocument24 pagesMedical Emergencies in Rehabilitation MedicineAzza El Awar100% (1)
- Electroconvulsive Therapy (ECT) PPT OdeDocument4 pagesElectroconvulsive Therapy (ECT) PPT OdeSatya IndraPas encore d'évaluation
- Basal Ganglia: Sridharan Neelamegan MMCDocument23 pagesBasal Ganglia: Sridharan Neelamegan MMCRetrocasualty Find OutPas encore d'évaluation
- Dr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityDocument41 pagesDr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityredderdatPas encore d'évaluation
- My Basal GangliaDocument18 pagesMy Basal GangliaPriya GKPas encore d'évaluation
- AIDS Dementia Complex (PowerPoint)Document39 pagesAIDS Dementia Complex (PowerPoint)tamaraoperadiva67% (3)
- UW Notes - 13 - PsychiatryDocument21 pagesUW Notes - 13 - PsychiatryDor BenayounPas encore d'évaluation
- ECTDocument24 pagesECTEdgar ManoodPas encore d'évaluation
- Psychiatry: ' ' Psychology 538 ' Pathology 540 ' Pharmacology 556Document24 pagesPsychiatry: ' ' Psychology 538 ' Pathology 540 ' Pharmacology 556Brush LowdryPas encore d'évaluation
- Electroconvulsive Therapy.9780195148206.29298Document481 pagesElectroconvulsive Therapy.9780195148206.29298aanchalPas encore d'évaluation
- DeliriumDocument27 pagesDeliriumBushra EjazPas encore d'évaluation
- INTRODUCTION TO NEUROPHARMACOLOGYyyDocument27 pagesINTRODUCTION TO NEUROPHARMACOLOGYyyEbad RazviPas encore d'évaluation
- Psychiatry Student Guide: MEDD 421 Clinical Skills 2019-2020Document25 pagesPsychiatry Student Guide: MEDD 421 Clinical Skills 2019-2020Rubie Ann TillorPas encore d'évaluation
- Process of Rehabilitation in PsychiatryDocument29 pagesProcess of Rehabilitation in PsychiatryRahul Kumar DiwakarPas encore d'évaluation
- PsychosisDocument32 pagesPsychosisRamya Gopala KrishnanPas encore d'évaluation
- Medical Mimics 2016Document24 pagesMedical Mimics 2016Susan Redmond-VaughtPas encore d'évaluation
- Antithrombotic Therapy For VTE Disease CHEST Guideline and Expert Panel ReportDocument38 pagesAntithrombotic Therapy For VTE Disease CHEST Guideline and Expert Panel ReportAdriana VasilicaPas encore d'évaluation
- Mneumonics PsychDxDocument7 pagesMneumonics PsychDxSuraj MukatiraPas encore d'évaluation
- Oebps 21Document91 pagesOebps 21Max Laban Seminario0% (1)
- Technological Advances in PsychiatryDocument48 pagesTechnological Advances in Psychiatryparth_sarathyPas encore d'évaluation
- Delirium Pathway - OTLPCM002-3Document1 pageDelirium Pathway - OTLPCM002-3Iftida YatiPas encore d'évaluation
- Phenomenology and Classification of Dystonia - A Consensus Update (2013)Document11 pagesPhenomenology and Classification of Dystonia - A Consensus Update (2013)mysticmdPas encore d'évaluation
- Psychiatry DiagnosisDocument4 pagesPsychiatry DiagnosisdrqubitPas encore d'évaluation
- MAKING SENSE OF PSYCHIATRY: An Insecure ProfessionDocument24 pagesMAKING SENSE OF PSYCHIATRY: An Insecure ProfessionPaul Minot MDPas encore d'évaluation
- Morning Report: Supervisor Dr. Sabar P. Siregar, SP - KJDocument47 pagesMorning Report: Supervisor Dr. Sabar P. Siregar, SP - KJVike Poraddwita YuliantiPas encore d'évaluation
- Neurotransmitters in Schizophrenia: Dr. Adel El SheshaiDocument47 pagesNeurotransmitters in Schizophrenia: Dr. Adel El SheshaielvinegunawanPas encore d'évaluation
- Brain Stimulation in Psychiatry by Kellner PDFDocument1 pageBrain Stimulation in Psychiatry by Kellner PDFNajia ChoudhuryPas encore d'évaluation
- Conversion Disorder (2018)Document12 pagesConversion Disorder (2018)Maria Von ShaftPas encore d'évaluation
- Tranylcypromine in Mind Part II - Review of Clinical PH - 2017 - European Neuro PDFDocument18 pagesTranylcypromine in Mind Part II - Review of Clinical PH - 2017 - European Neuro PDFdanilomarandolaPas encore d'évaluation
- Localization of Brain Stem LesionsDocument35 pagesLocalization of Brain Stem LesionsHrishikesh Jha0% (1)
- Notes On PsychiatryDocument10 pagesNotes On PsychiatryMark VillenaPas encore d'évaluation
- Antipsychotic-Induced Extrapyramidal Syndromes andDocument144 pagesAntipsychotic-Induced Extrapyramidal Syndromes andSeiska Mega100% (1)
- Where There Is No PsychiatristDocument335 pagesWhere There Is No PsychiatristIFANI NURUL ISLAMYPas encore d'évaluation
- Psy 105 Neurological DisordersDocument11 pagesPsy 105 Neurological Disordersdesiree leornasPas encore d'évaluation
- Bad Guidelines Management of Adults With Delusional InfestationDocument18 pagesBad Guidelines Management of Adults With Delusional InfestationRBGBGB RBGPas encore d'évaluation
- Substance Abuse Disorders - GROUP 3Document96 pagesSubstance Abuse Disorders - GROUP 3Mary Christine IlangaPas encore d'évaluation
- Anti-Migraine DrugsDocument21 pagesAnti-Migraine DrugsGareth BalePas encore d'évaluation
- Receptors Ionchannel TransporterDocument58 pagesReceptors Ionchannel TransporterDeepu Vijay100% (1)
- Psychiatry Finals - Passport 2nd Edition For Lambert PDFDocument110 pagesPsychiatry Finals - Passport 2nd Edition For Lambert PDFDoctor ShathaPas encore d'évaluation
- Chest Pain PresentationDocument24 pagesChest Pain PresentationAnonymous 17awurSUPas encore d'évaluation
- Fibromyalgia A Clinical ReviewDocument9 pagesFibromyalgia A Clinical ReviewastrogliaPas encore d'évaluation
- JCP Optimizing Antipsychotics GuidelinesDocument31 pagesJCP Optimizing Antipsychotics GuidelinesSusasti HasanahPas encore d'évaluation
- Medicines in PregnancyDocument18 pagesMedicines in Pregnancymominur11Pas encore d'évaluation
- Psychiatry Case LogDocument6 pagesPsychiatry Case Logf3er3Pas encore d'évaluation
- Dementia: Diagnosis and TreatmentDocument53 pagesDementia: Diagnosis and Treatmentakashdeep050% (1)
- Treatment of Chronic Non Cancer Pain Lancet 2011Document10 pagesTreatment of Chronic Non Cancer Pain Lancet 2011jhonjrodriPas encore d'évaluation
- HIV and Mental HealthDocument7 pagesHIV and Mental HealthAyu RajikanPas encore d'évaluation
- The Management of Common and Selected Psychiatric EmergenciesDocument129 pagesThe Management of Common and Selected Psychiatric EmergenciesHasaan Khan100% (1)
- Vitamins: (DR Pauling Recommendation, Svaki Dan Uzeti)Document3 pagesVitamins: (DR Pauling Recommendation, Svaki Dan Uzeti)Veky VictoriaPas encore d'évaluation
- NCLEX Questions 96-105Document3 pagesNCLEX Questions 96-105kxviperPas encore d'évaluation
- Evidence Based Radiation Oncology PDFDocument2 pagesEvidence Based Radiation Oncology PDFDavone0% (2)
- NCP Ineffective Airway ClearanceDocument5 pagesNCP Ineffective Airway ClearanceArt Christian Ramos100% (1)
- Medication Calculation Practice Problems: Level Ii, Iii and IvDocument6 pagesMedication Calculation Practice Problems: Level Ii, Iii and IvQueennita100% (7)
- Counseling Children With Emotional DisturbanceDocument15 pagesCounseling Children With Emotional DisturbanceLaKenya BrowderPas encore d'évaluation
- BF Skinner Written ReportDocument3 pagesBF Skinner Written ReportKen TalkPas encore d'évaluation
- Hyperurecimia and GoutDocument3 pagesHyperurecimia and GoutSunshine_Bacla_4275Pas encore d'évaluation
- Englishwritten Released 2018 PDFDocument401 pagesEnglishwritten Released 2018 PDFbobobo96Pas encore d'évaluation
- Coagulation DisordersDocument26 pagesCoagulation DisordersLia pramita0% (1)
- Transgender SpeechDocument61 pagesTransgender Speechjreljosh1994100% (1)
- NaturopathyDocument47 pagesNaturopathyDeenky ShahPas encore d'évaluation
- Test Bank For Issues and Ethics in The Helping Professions 8th EditionDocument12 pagesTest Bank For Issues and Ethics in The Helping Professions 8th EditionCorey Vargas100% (2)
- Rehabilitation of Leprosy (Lecture 28 Mei 2018)Document49 pagesRehabilitation of Leprosy (Lecture 28 Mei 2018)Firdiana Ardianti100% (1)
- Chapter 11 Management of Hydrocarbon PoisoningDocument2 pagesChapter 11 Management of Hydrocarbon Poisoningarief muhammadPas encore d'évaluation
- Master in Clinical PharmacyDocument2 pagesMaster in Clinical PharmacytktPas encore d'évaluation
- Joint Replacement KolkataDocument15 pagesJoint Replacement KolkataKoushik MondalPas encore d'évaluation
- Bellak and Meyers Ego Function Assessment 1975 Newer Copy 2Document25 pagesBellak and Meyers Ego Function Assessment 1975 Newer Copy 2Janine Michelle SyPas encore d'évaluation
- Asthma by ConsensusDocument87 pagesAsthma by ConsensusSatnam KaurPas encore d'évaluation
- Nonvital Pulp Therapy On Primary TeethDocument15 pagesNonvital Pulp Therapy On Primary TeethJose RoldanPas encore d'évaluation
- Roland Joseph Reyes Toledo, RM, RN, ET: Qualifications SummaryDocument4 pagesRoland Joseph Reyes Toledo, RM, RN, ET: Qualifications SummaryGlobal medik indonesiaPas encore d'évaluation
- Pharmacology of The GITDocument31 pagesPharmacology of The GITmarviecute22Pas encore d'évaluation
- OT Sample Exam QuestionsDocument4 pagesOT Sample Exam Questionsagatha2108Pas encore d'évaluation
- 10 1 1 823 6398 PDFDocument5 pages10 1 1 823 6398 PDFDian Novita AnggraeniPas encore d'évaluation
- Guidance Office Referral FormDocument2 pagesGuidance Office Referral FormHainee Caoile-MinasPas encore d'évaluation
- Pseudomonarchia DaemonumDocument7 pagesPseudomonarchia DaemonumManuel AlorPas encore d'évaluation
- Bipolar Brochure English FINAL 150109 PDFDocument9 pagesBipolar Brochure English FINAL 150109 PDFIka M. HendrajayaPas encore d'évaluation
- Siddha Applied Science InstituteDocument4 pagesSiddha Applied Science InstituteLagin DranPas encore d'évaluation
- Concurrent Sem 1Document18 pagesConcurrent Sem 1Jona D'john100% (1)
- Addressing Anxiety in School SettingsDocument15 pagesAddressing Anxiety in School Settingssimona corneaPas encore d'évaluation