Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Using The Edinburgh Gait Score PDFDocument8 pagesUsing The Edinburgh Gait Score PDFCamila Solange100% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Kizen Sheiko 3 Day - Cycle 1Document61 pagesKizen Sheiko 3 Day - Cycle 1Dimitris OurdasPas encore d'évaluation
- Sleep QualityDocument8 pagesSleep QualityRidwan AdiansyahPas encore d'évaluation
- Obsessive-Compulsive Disorder in Children and Adolescents: Georgina Krebs, Isobel HeymanDocument5 pagesObsessive-Compulsive Disorder in Children and Adolescents: Georgina Krebs, Isobel HeymanRidwan AdiansyahPas encore d'évaluation
- Forensic Medical Examination of Victims of Trafficking in Human BeingsDocument5 pagesForensic Medical Examination of Victims of Trafficking in Human BeingsRidwan AdiansyahPas encore d'évaluation
- Diet Penyakit Hati: - Dr. Joko Wahyu Wibowo, MkesDocument49 pagesDiet Penyakit Hati: - Dr. Joko Wahyu Wibowo, MkesRidwan AdiansyahPas encore d'évaluation
- Kinesiology For Occupational Therapy-32-50Document19 pagesKinesiology For Occupational Therapy-32-50birjuPas encore d'évaluation
- TX of Colles FXDocument4 pagesTX of Colles FXJessica CaronPas encore d'évaluation
- Levels of AmputationsDocument6 pagesLevels of AmputationsJuanitoCabatañaLimIII100% (1)
- Comparative Study of Functional Outcome of Acl Reconstruction by Hamstring VS Peroneus Longus AutograftDocument12 pagesComparative Study of Functional Outcome of Acl Reconstruction by Hamstring VS Peroneus Longus AutograftIJAR JOURNALPas encore d'évaluation
- Gait Deviations in Orthotics & ProstheticsDocument10 pagesGait Deviations in Orthotics & ProstheticsJulia SalvioPas encore d'évaluation
- Jazzercise Setfor Valentines 02062011Document24 pagesJazzercise Setfor Valentines 02062011Hailey JohnstonPas encore d'évaluation
- Abbas Diss 2011Document5 pagesAbbas Diss 2011yayu latifahPas encore d'évaluation
- Rehab Grand Rounds: Comprehensive Approach To The Management of Scapular Dyskinesia in The Overhead Throwing AthleteDocument8 pagesRehab Grand Rounds: Comprehensive Approach To The Management of Scapular Dyskinesia in The Overhead Throwing AthletekotraePas encore d'évaluation
- Return To Play Following Anterior Shoulder Dislocation and Stabilization SurgeryDocument17 pagesReturn To Play Following Anterior Shoulder Dislocation and Stabilization SurgerydrjorgewtorresPas encore d'évaluation
- Open and Closed Packed Positions of JointsDocument1 pageOpen and Closed Packed Positions of JointsRaymond100% (4)
- Kinematics of Knee JointDocument16 pagesKinematics of Knee JointnttangPas encore d'évaluation
- Chondromalacia Patella - Causes & Treatment - Knee Pain ExplainedDocument5 pagesChondromalacia Patella - Causes & Treatment - Knee Pain ExplainedJames MukhwanaPas encore d'évaluation
- Compilation of Netters Illustrations Moores Tables and SnellDocument50 pagesCompilation of Netters Illustrations Moores Tables and SnellAyres EvangPas encore d'évaluation
- Pe 1Document11 pagesPe 1Patrickjohn GelilioPas encore d'évaluation
- Lauge Hansen ClassificationDocument3 pagesLauge Hansen ClassificationallybishPas encore d'évaluation
- Oral Dislocation Rehabilitation Program - FirstDocument2 pagesOral Dislocation Rehabilitation Program - FirstPriyaki SebastianPas encore d'évaluation
- Bones and Joints of Upper LimbDocument34 pagesBones and Joints of Upper LimbNisreen SalamePas encore d'évaluation
- ShoulderDocument17 pagesShoulderNehaPas encore d'évaluation
- ACL Mahmud OPD PatientDocument16 pagesACL Mahmud OPD PatientDrMizanur RahmanPas encore d'évaluation
- Knee Special TestDocument89 pagesKnee Special TestNURUL AFIQAH NORKHAMISZANPas encore d'évaluation
- 36 Pictures To See Which Muscle You'Re Stretching - Be Young Be GreenDocument13 pages36 Pictures To See Which Muscle You'Re Stretching - Be Young Be GreenMarco TorrePas encore d'évaluation
- Transtibial Acl Reconstruction For BTB GraftsDocument6 pagesTranstibial Acl Reconstruction For BTB GraftsJose SantiagoPas encore d'évaluation
- Full Body BurnerDocument4 pagesFull Body BurnerErica JanssonPas encore d'évaluation
- Anatomi CrossectionalDocument12 pagesAnatomi CrossectionalRamaNurullarifahPas encore d'évaluation
- Naik, S. - Biomechanics of Knee ComplexDocument25 pagesNaik, S. - Biomechanics of Knee ComplexKyle Bois100% (4)
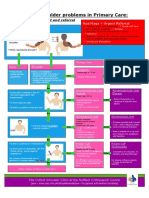
- NHS UK Diagnosis of Shoulder ProblemsDocument1 pageNHS UK Diagnosis of Shoulder ProblemsmertPas encore d'évaluation
- Subtalar JointDocument8 pagesSubtalar JointkotraePas encore d'évaluation
- Module ADocument37 pagesModule AdumpyforhimPas encore d'évaluation