Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- 1H06B Lectures 1-4 Review CardiacDocument16 pages1H06B Lectures 1-4 Review Cardiachaaris 7khanPas encore d'évaluation
- CURRICULUM-MAP 1st Quarter Science 9Document4 pagesCURRICULUM-MAP 1st Quarter Science 9maria ana rehmontessori100% (2)
- Modul 1. Patofisiologi ACSDocument24 pagesModul 1. Patofisiologi ACSFadhilAfifPas encore d'évaluation
- Chapter 9 - Transport in AnimalsDocument6 pagesChapter 9 - Transport in AnimalsLeann LeePas encore d'évaluation
- Tadano Hydraulic Crane Ar 1000m 1 p2 1ej Parts Catalog EnjpDocument22 pagesTadano Hydraulic Crane Ar 1000m 1 p2 1ej Parts Catalog Enjprachelharrison091289kdj100% (103)
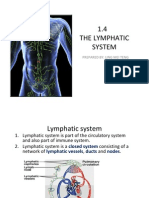
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDocument15 pages1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingPas encore d'évaluation
- Physical Assessment of Cardiovascular SystemDocument31 pagesPhysical Assessment of Cardiovascular SystemaagPas encore d'évaluation
- BT Training ManualDocument140 pagesBT Training ManualYvonne Pearl Delos Santos100% (1)
- Cardiac Cycle: DR Nilesh Kate MBBS, MD Associate Prof Esic Medical College, Gulbarga. Dept. of PhysiologyDocument41 pagesCardiac Cycle: DR Nilesh Kate MBBS, MD Associate Prof Esic Medical College, Gulbarga. Dept. of Physiologyabdullah irpanPas encore d'évaluation
- Activity On Circulatory SystemDocument2 pagesActivity On Circulatory SystemChin CustodioPas encore d'évaluation
- Cardiovascular System PDFDocument71 pagesCardiovascular System PDFramadanPas encore d'évaluation
- ACC-AHA Guidelines Heart FailureDocument56 pagesACC-AHA Guidelines Heart FailureUswatul HasanahPas encore d'évaluation
- Introduction To High Risk PregnancyDocument13 pagesIntroduction To High Risk PregnancyMabes100% (1)
- UACE BIOLOGY PAPER 1 2005 Marking GuideDocument28 pagesUACE BIOLOGY PAPER 1 2005 Marking GuideKbale michealPas encore d'évaluation
- Oxford Science Fact File 3 Teaching GuideDocument96 pagesOxford Science Fact File 3 Teaching GuideAdnan Roonjha50% (10)
- Circulatory System Diseases QuizDocument3 pagesCirculatory System Diseases QuizMaruja RuizPas encore d'évaluation
- Medical Terminology For Health Professions 7th Edition Ehrlich Test Bank 1Document8 pagesMedical Terminology For Health Professions 7th Edition Ehrlich Test Bank 1leroy100% (50)
- Presentation BP MonitorDocument7 pagesPresentation BP MonitorImwaniki21Pas encore d'évaluation
- Some Notes For IGCSE BiologyDocument38 pagesSome Notes For IGCSE BiologylauraPas encore d'évaluation
- Blood Supply of The Heart & Conduction System: Dr. Nabil KhouriDocument37 pagesBlood Supply of The Heart & Conduction System: Dr. Nabil KhouriDefyna Dwi LestariPas encore d'évaluation
- Soal Inggris - 2Document6 pagesSoal Inggris - 2vivitrisami05Pas encore d'évaluation
- A New Echocardiographic Window To Visualize The Mitral Valve Complex During Mitral Valve Repair For Functional Mitral RegurgitationDocument3 pagesA New Echocardiographic Window To Visualize The Mitral Valve Complex During Mitral Valve Repair For Functional Mitral Regurgitationricardo villaPas encore d'évaluation
- Human Embryology:: Heart Development IIDocument46 pagesHuman Embryology:: Heart Development IIHanifah ZainPas encore d'évaluation
- Hopkins Status ReportDocument56 pagesHopkins Status ReportJeffrey GillespiePas encore d'évaluation
- Massage Skill: Indications and Contra-IndicationsDocument4 pagesMassage Skill: Indications and Contra-IndicationsAmimul EhsanPas encore d'évaluation
- Heart Disease: Symptoms of Heart Disease in Your Blood Vessels (Atherosclerotic Disease)Document22 pagesHeart Disease: Symptoms of Heart Disease in Your Blood Vessels (Atherosclerotic Disease)Kenneth Jay EdnacoPas encore d'évaluation
- Test Bank For Ecg Essentials of Electrocardiography 1st Edition by SotoDocument36 pagesTest Bank For Ecg Essentials of Electrocardiography 1st Edition by Sotogrinting.creation4qlo100% (48)
- San Vicente West, Urdaneta CityDocument5 pagesSan Vicente West, Urdaneta CityTIPAY, EMELIE L.Pas encore d'évaluation
- Non Hodgkin's LymphomaDocument31 pagesNon Hodgkin's LymphomaJeo Thomas100% (1)
- The Fontan Circulation Contin EducDocument5 pagesThe Fontan Circulation Contin EducAishu BPas encore d'évaluation