Vous aimerez peut-être aussi
- Homework Helpers - Chemistry PDFDocument311 pagesHomework Helpers - Chemistry PDFTamby100% (1)
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtD'EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtÉvaluation : 5 sur 5 étoiles5/5 (1)
- Stroke: A.K.A. Cerebrovascular Accident (CVA) & Brain AttackDocument81 pagesStroke: A.K.A. Cerebrovascular Accident (CVA) & Brain AttackNovianty GliceriaPas encore d'évaluation
- 2nd Semester All Courses-100Document194 pages2nd Semester All Courses-100Ejiade PeterPas encore d'évaluation
- Acute Stroke Management by Carlos L ChuaDocument61 pagesAcute Stroke Management by Carlos L ChuaRemaica Hernadez100% (1)
- SLEDocument42 pagesSLETrishenth FonsekaPas encore d'évaluation
- Real Talk GrammarDocument237 pagesReal Talk GrammarOmar yoshiPas encore d'évaluation
- StrokeDocument66 pagesStrokeJoshua Smith100% (1)
- Welding Defects and AcceptanceDocument76 pagesWelding Defects and Acceptancearavindan100% (1)
- Traumatic Brain Injury PresentationDocument51 pagesTraumatic Brain Injury PresentationKah Sui Tan100% (2)
- The Premature BabyDocument92 pagesThe Premature BabyTrishenth Fonseka100% (1)
- Ammonia Tech Manual 2002Document28 pagesAmmonia Tech Manual 2002Talha Bin Zubair0% (1)
- Stroke Lecture PDFDocument41 pagesStroke Lecture PDFPAK DHEPas encore d'évaluation
- Cerebrovascular AccidentDocument79 pagesCerebrovascular AccidentKathy B. AbuanPas encore d'évaluation
- Stroke Syndromes and Localization 2007Document56 pagesStroke Syndromes and Localization 2007SaintPaul Univ100% (1)
- Arrhythmia: PalpitationDocument36 pagesArrhythmia: PalpitationHala BahaaPas encore d'évaluation
- Lea 2 PDFDocument21 pagesLea 2 PDFKY Renz100% (1)
- COMPRESSED AIR VALIDATION SYSTEMDocument13 pagesCOMPRESSED AIR VALIDATION SYSTEMbpharmba100% (5)
- Angelito L. Ramos Jr. RN Clinical InstructorDocument68 pagesAngelito L. Ramos Jr. RN Clinical Instructorraymondblade18100% (17)
- Cerebrovascular Accident CVADocument8 pagesCerebrovascular Accident CVAFlora Angeli PastoresPas encore d'évaluation
- 1228 HFStroke Altered Neuro 2011Document74 pages1228 HFStroke Altered Neuro 2011Cyndy EnterlinePas encore d'évaluation
- Ischemic StrokeDocument20 pagesIschemic StrokeMargaret BalePas encore d'évaluation
- Management of Stroke: in The Name of God The Most Gracious The Most MercifulDocument29 pagesManagement of Stroke: in The Name of God The Most Gracious The Most MercifulHaider Nadhem AL-rubaiPas encore d'évaluation
- CVA (Dr. Kwasa)Document23 pagesCVA (Dr. Kwasa)Uzma KhanPas encore d'évaluation
- TutorialDocument18 pagesTutorialEllya Syahfitri 2108125983Pas encore d'évaluation
- AHA/ASA Guideline - 2007 Guidelines For The Early Management of Adults With Ischemia StrokeDocument8 pagesAHA/ASA Guideline - 2007 Guidelines For The Early Management of Adults With Ischemia StrokeJadwiga O'GormanPas encore d'évaluation
- ISCHAEMIC STROKE GUIDEDocument59 pagesISCHAEMIC STROKE GUIDEVenosha GunasekaranPas encore d'évaluation
- Cva Swiss Bell HotelDocument80 pagesCva Swiss Bell HotelKumbendy Sada0% (1)
- Intracranial Hypertension: Miroslav GajdošDocument30 pagesIntracranial Hypertension: Miroslav GajdošKobi DabushPas encore d'évaluation
- Stroke: Presence Regional EMS System September 2013Document72 pagesStroke: Presence Regional EMS System September 2013AniPas encore d'évaluation
- Cerebro Vascular DiseaseDocument25 pagesCerebro Vascular DiseaseMuhammad Asif NizamiPas encore d'évaluation
- Electroconvulsive Therapy: An UpdateDocument39 pagesElectroconvulsive Therapy: An UpdateAnonymous 83o62cPas encore d'évaluation
- Cerebrovascular AccidentDocument37 pagesCerebrovascular AccidentEguia NielPas encore d'évaluation
- Dr. Riki Sukiandra, SPS - Acute Stroke Diagnosis and Management in Primary Health CareDocument41 pagesDr. Riki Sukiandra, SPS - Acute Stroke Diagnosis and Management in Primary Health CareNurRahMatPas encore d'évaluation
- Krisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranDocument85 pagesKrisis Hypertensi: Sigit Widyatmoko Fakultas KedokteranSeptian WidiantoPas encore d'évaluation
- CVA SsDocument39 pagesCVA SsAnushri ManePas encore d'évaluation
- StrokeDocument34 pagesStrokeMakojoa KatisoPas encore d'évaluation
- Cerebrovascular Accident Types, Causes, Signs, and ManagementDocument5 pagesCerebrovascular Accident Types, Causes, Signs, and ManagementPrakuz Harmony SubedifiedPas encore d'évaluation
- Stroke Syndrome - BenyDocument22 pagesStroke Syndrome - BenyyericosabathinoPas encore d'évaluation
- Understanding Syncope: Causes, Diagnosis and TreatmentDocument44 pagesUnderstanding Syncope: Causes, Diagnosis and TreatmentSap ModulesPas encore d'évaluation
- Acute Stroke Lecture (Fall 2021) 2Document47 pagesAcute Stroke Lecture (Fall 2021) 2shahad alghamdiPas encore d'évaluation
- CVA Card (Simple 7)Document2 pagesCVA Card (Simple 7)Scotty SpurlinPas encore d'évaluation
- Cerebrovascular Accident (Stroke, Brain Attack)Document29 pagesCerebrovascular Accident (Stroke, Brain Attack)Xer AlliuqPas encore d'évaluation
- Hypertension & End Organ DamageDocument41 pagesHypertension & End Organ DamageTrushank PathakPas encore d'évaluation
- Approach To Patient With Syncope: Iman Sulaiman Al-HatmiDocument49 pagesApproach To Patient With Syncope: Iman Sulaiman Al-HatmiAlexandru CozmaPas encore d'évaluation
- Transient Ischemic AttacksDocument10 pagesTransient Ischemic AttacksfabianounifenasPas encore d'évaluation
- ER & CCU ProtocolDocument14 pagesER & CCU ProtocolatinafansifPas encore d'évaluation
- Anesthesia For Neurosurg2Document42 pagesAnesthesia For Neurosurg2Praveen RamasamyPas encore d'évaluation
- Fundamentals of Stroke and TIADocument12 pagesFundamentals of Stroke and TIAMaria WibawaPas encore d'évaluation
- Emergencies in GP DR Ibrahim AlmoosaDocument70 pagesEmergencies in GP DR Ibrahim Almoosaموسى التميميPas encore d'évaluation
- Cerebrovascular Disease: Departemen Neurologi Fakultas Kedokteran Universitas Islam Sumatera UtaraDocument48 pagesCerebrovascular Disease: Departemen Neurologi Fakultas Kedokteran Universitas Islam Sumatera UtaraismihabPas encore d'évaluation
- Case 5 NotesDocument16 pagesCase 5 NotesA MPas encore d'évaluation
- CNS M1 Lecture Slides Compiled, DR OsaiDocument185 pagesCNS M1 Lecture Slides Compiled, DR OsaiMusaPas encore d'évaluation
- Brain Attack: NR-75D Diana Diaz RN, MSDocument66 pagesBrain Attack: NR-75D Diana Diaz RN, MSJoshua SmithPas encore d'évaluation
- CvaDocument42 pagesCvad_94Pas encore d'évaluation
- Cerebro-Vascular Disease & Stroke: Faizan Zaffar KashooDocument57 pagesCerebro-Vascular Disease & Stroke: Faizan Zaffar KashooDrGasnasPas encore d'évaluation
- 5A. Traumatic Brain InjuriesDocument242 pages5A. Traumatic Brain InjuriesMajed AlamiPas encore d'évaluation
- Stroke Hemoragik: Yuneldi Anwar Sps Departemen Neurologi FK UsuDocument28 pagesStroke Hemoragik: Yuneldi Anwar Sps Departemen Neurologi FK UsuDwi Meutia IndriatiPas encore d'évaluation
- Subarachnoid Hemorrhage With AneurysymDocument30 pagesSubarachnoid Hemorrhage With AneurysymmunaPas encore d'évaluation
- CVA Case StudyDocument4 pagesCVA Case Studynbk08Pas encore d'évaluation
- Clinical Presentation of Cerebrovascular Disease: David Griesemer, MDDocument47 pagesClinical Presentation of Cerebrovascular Disease: David Griesemer, MDPedro CedeñoPas encore d'évaluation
- Stroke 151227140046Document84 pagesStroke 151227140046MunnaPas encore d'évaluation
- Hypertensive Crisis ManagementDocument27 pagesHypertensive Crisis ManagementDian Puspa100% (1)
- DR Mohamed A. Fathi Cardiology Specialist and Tutor GMCHRCDocument76 pagesDR Mohamed A. Fathi Cardiology Specialist and Tutor GMCHRCMohamed Ahmed FathiPas encore d'évaluation
- Case-Based Device Therapy for Heart FailureD'EverandCase-Based Device Therapy for Heart FailureUlrika Birgersdotter-GreenPas encore d'évaluation
- Guide to Canine and Feline ElectrocardiographyD'EverandGuide to Canine and Feline ElectrocardiographyRuth WillisPas encore d'évaluation
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideD'EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuidePas encore d'évaluation
- Quarterly Report On Case FindingDocument2 pagesQuarterly Report On Case FindingTrishenth FonsekaPas encore d'évaluation
- Quarterly Report On Sputum Conversion of Positive Patients at The End of Intensive PhaseDocument1 pageQuarterly Report On Sputum Conversion of Positive Patients at The End of Intensive PhaseTrishenth FonsekaPas encore d'évaluation
- National TB Control ManualDocument223 pagesNational TB Control ManualTrishenth FonsekaPas encore d'évaluation
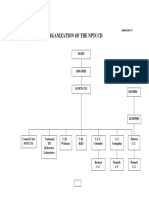
- Organization of NPTCCD PDFDocument2 pagesOrganization of NPTCCD PDFTrishenth FonsekaPas encore d'évaluation
- Quarterly Report On TB and non-TB WardsDocument3 pagesQuarterly Report On TB and non-TB WardsTrishenth FonsekaPas encore d'évaluation
- Duties of MOHDocument3 pagesDuties of MOHTrishenth FonsekaPas encore d'évaluation
- Quarterly Report On The Results of Treatment of Patients Registered 12-15 Months EarlierDocument2 pagesQuarterly Report On The Results of Treatment of Patients Registered 12-15 Months EarlierTrishenth FonsekaPas encore d'évaluation
- Quarterly Report On Microscopic Activities and LogisticsDocument2 pagesQuarterly Report On Microscopic Activities and LogisticsTrishenth FonsekaPas encore d'évaluation
- Quarterly Report On Program ManagementDocument7 pagesQuarterly Report On Program ManagementTrishenth FonsekaPas encore d'évaluation
- Register of TB SuspectsDocument1 pageRegister of TB SuspectsTrishenth FonsekaPas encore d'évaluation
- National TB RegisterDocument2 pagesNational TB RegisterTrishenth FonsekaPas encore d'évaluation
- Laborotory Manual For Tuberculosis ControlDocument5 pagesLaborotory Manual For Tuberculosis ControlTrishenth FonsekaPas encore d'évaluation
- Living With AFib Patient GuideDocument73 pagesLiving With AFib Patient GuideTrishenth FonsekaPas encore d'évaluation
- Lab Form For Sputum Examination PDFDocument1 pageLab Form For Sputum Examination PDFTrishenth FonsekaPas encore d'évaluation
- 29 - Heart Disease Complicating PregnancyDocument18 pages29 - Heart Disease Complicating PregnancyTrishenth FonsekaPas encore d'évaluation
- QuotesDocument1 pageQuotesTrishenth FonsekaPas encore d'évaluation
- Paediatric UrologyDocument194 pagesPaediatric UrologyTrishenth FonsekaPas encore d'évaluation
- Neck Pain and Pain Down The ArmDocument27 pagesNeck Pain and Pain Down The ArmTrishenth FonsekaPas encore d'évaluation
- 12 - Medical NegligenceDocument34 pages12 - Medical NegligenceTrishenth FonsekaPas encore d'évaluation
- 15 - CN Poisoning 2Document2 pages15 - CN Poisoning 2Trishenth FonsekaPas encore d'évaluation
- Medical Ethics Code ExplainedDocument23 pagesMedical Ethics Code ExplainedTrishenth FonsekaPas encore d'évaluation
- Gas Poisoning (Irrespirable Gases) : Asphyxial DeathDocument5 pagesGas Poisoning (Irrespirable Gases) : Asphyxial DeathTrishenth FonsekaPas encore d'évaluation
- 11 - Professional SecrecyDocument10 pages11 - Professional SecrecyTrishenth Fonseka100% (1)
- 08 - Post Mortem InstrumentsDocument6 pages08 - Post Mortem InstrumentsTrishenth FonsekaPas encore d'évaluation
- 13 - Medicolegal Duties of A DoctorDocument13 pages13 - Medicolegal Duties of A DoctorTrishenth FonsekaPas encore d'évaluation
- SLMC - Regulating Sri Lanka's Medical ProfessionDocument27 pagesSLMC - Regulating Sri Lanka's Medical ProfessionTrishenth FonsekaPas encore d'évaluation
- 10 - Introduction To Legal System in SLDocument6 pages10 - Introduction To Legal System in SLTrishenth FonsekaPas encore d'évaluation
- 09 - Changes After Death and Time Since DeathDocument9 pages09 - Changes After Death and Time Since DeathTrishenth FonsekaPas encore d'évaluation
- Omcmle Physiology Workbook Part 5 PDFDocument63 pagesOmcmle Physiology Workbook Part 5 PDFloiuse shepiralPas encore d'évaluation
- 32776Document6 pages32776Muqtar KhanPas encore d'évaluation
- Torn MeniscusDocument10 pagesTorn MeniscusKrystal Veverka100% (3)
- HSS Article LimitState Plastification 0718 060120Document3 pagesHSS Article LimitState Plastification 0718 060120clam2014Pas encore d'évaluation
- Chefs at HomeDocument4 pagesChefs at Homezbdv2kyzv7Pas encore d'évaluation
- Ben Wilkins PRISON MADNESS and LOVE LETTERS: THE LOST ARTDocument5 pagesBen Wilkins PRISON MADNESS and LOVE LETTERS: THE LOST ARTBarbara BergmannPas encore d'évaluation
- 692pu 6 6Document1 page692pu 6 6Diego GodoyPas encore d'évaluation
- Lesson 1.5: Measurements of Directions and Angles: Unit IDocument12 pagesLesson 1.5: Measurements of Directions and Angles: Unit ICarlo CabanusPas encore d'évaluation
- Traxonecue Catalogue 2011 Revise 2 Low Res Eng (4!5!2011)Document62 pagesTraxonecue Catalogue 2011 Revise 2 Low Res Eng (4!5!2011)Wilson ChimPas encore d'évaluation
- Return SectionDocument1 pageReturn SectionDaniel Pouso DiosPas encore d'évaluation
- Shiva Home - DCFDocument2 pagesShiva Home - DCFshyamsundar_cePas encore d'évaluation
- Biology Standard XII Human Reproduction WorksheetDocument10 pagesBiology Standard XII Human Reproduction WorksheetPriya SinghPas encore d'évaluation
- ASSIGNMENTDocument10 pagesASSIGNMENTKoleen Lopez ÜPas encore d'évaluation
- Systematic Literature Review and Mapping of The Prediction of Pile CapacitiesDocument12 pagesSystematic Literature Review and Mapping of The Prediction of Pile CapacitiesCaio Augusto Lemke CostaPas encore d'évaluation
- Weekly Report 52Document196 pagesWeekly Report 52Erceanu DanPas encore d'évaluation
- Fossil Fuel and The Environment PPT Project FinalDocument14 pagesFossil Fuel and The Environment PPT Project Finalapi-298052133Pas encore d'évaluation
- Function and Definite Integrals ExplainedDocument7 pagesFunction and Definite Integrals Explainedana maharaniPas encore d'évaluation
- This Is Your Presentation TitleDocument28 pagesThis Is Your Presentation TitleStephanie AcarapiPas encore d'évaluation
- Sing 2Document64 pagesSing 2WindsurfingFinnPas encore d'évaluation
- 0580 w15 QP 42Document16 pages0580 w15 QP 42Shahrizan Noor100% (1)
- Scheme of Valuation and Key for Transportation Engineering ExamDocument3 pagesScheme of Valuation and Key for Transportation Engineering ExamSivakumarPas encore d'évaluation
- October 14, 2011 Strathmore TimesDocument28 pagesOctober 14, 2011 Strathmore TimesStrathmore TimesPas encore d'évaluation
- Đánh giá chế độ ăn kiêng: Nhịn ăn gián đoạn để giảm cân- wed HarvardDocument14 pagesĐánh giá chế độ ăn kiêng: Nhịn ăn gián đoạn để giảm cân- wed HarvardNam NguyenHoangPas encore d'évaluation