Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Apocrine Carcinoma of The BreastDocument18 pagesApocrine Carcinoma of The BreastOscar HalumPas encore d'évaluation
- Completion Thyroidectomy in Differentiated Thyroid Cancer - When To PerformDocument4 pagesCompletion Thyroidectomy in Differentiated Thyroid Cancer - When To PerformOscar HalumPas encore d'évaluation
- Gri Bovs Kaja Rupp 2016Document8 pagesGri Bovs Kaja Rupp 2016Kike MendozaPas encore d'évaluation
- Mucinous Neoplasms of The Appendix - A Current Comprehensive Clinicopathologic and Imaging ReviewDocument12 pagesMucinous Neoplasms of The Appendix - A Current Comprehensive Clinicopathologic and Imaging ReviewOscar HalumPas encore d'évaluation
- Closure Methods For Laparotomy Incisions For Preventing Incisional Hernias and Other Wound ComplicationsDocument169 pagesClosure Methods For Laparotomy Incisions For Preventing Incisional Hernias and Other Wound ComplicationsOscar HalumPas encore d'évaluation
- Coincidence of Thymoma and Breast Cancer in A 56 Year Old FemaleDocument7 pagesCoincidence of Thymoma and Breast Cancer in A 56 Year Old FemaleOscar HalumPas encore d'évaluation
- Role of Postoperative Radiotherapy in Dermatofibrosarcoma ProtuberansDocument8 pagesRole of Postoperative Radiotherapy in Dermatofibrosarcoma ProtuberansOscar HalumPas encore d'évaluation
- Mucinous Cystic Neoplasm of The Pancreas Is Not An Aggressive EntityDocument19 pagesMucinous Cystic Neoplasm of The Pancreas Is Not An Aggressive EntityOscar HalumPas encore d'évaluation
- Management of Esophageal Caustic InjuryDocument10 pagesManagement of Esophageal Caustic InjuryOscar HalumPas encore d'évaluation
- ATA Tiroides PDFDocument133 pagesATA Tiroides PDFGloria Pg MontzePas encore d'évaluation
- Clear Cell CADocument2 pagesClear Cell CAOscar HalumPas encore d'évaluation
- ISBI Guidelines For Burn CareDocument69 pagesISBI Guidelines For Burn CareOscar HalumPas encore d'évaluation
- Final Clear CellDocument9 pagesFinal Clear CellOscar HalumPas encore d'évaluation
- Upload 1Document1 pageUpload 1Oscar HalumPas encore d'évaluation
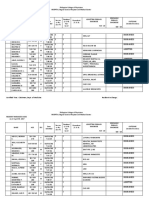
- Philippine College of Physicians Resident Managed CasesDocument6 pagesPhilippine College of Physicians Resident Managed CasesOscar HalumPas encore d'évaluation
- Mebo OintmentDocument17 pagesMebo OintmentFarahPas encore d'évaluation
- Upload 2Document1 pageUpload 2Oscar HalumPas encore d'évaluation
- Recent Trends in Burn Epidemiology WorldwideDocument1 pageRecent Trends in Burn Epidemiology WorldwideOscar HalumPas encore d'évaluation
- Tbguide PDFDocument44 pagesTbguide PDFOscar HalumPas encore d'évaluation
- ATP III Guideline KolesterolDocument6 pagesATP III Guideline KolesterolRakasiwi GalihPas encore d'évaluation
- Cap Guidelines Booklet 2010 UpdateDocument101 pagesCap Guidelines Booklet 2010 UpdateIcko DinopolPas encore d'évaluation
- SOAPDocument5 pagesSOAPOscar HalumPas encore d'évaluation
- RotavirusDocument13 pagesRotavirusOscar HalumPas encore d'évaluation
- ReserpineDocument3 pagesReserpineOscar HalumPas encore d'évaluation
- GP 96Document24 pagesGP 96Study MaterialPas encore d'évaluation
- GYNE 5.01 - Neoplastic Disease of The Ovary - Dr. TinioDocument7 pagesGYNE 5.01 - Neoplastic Disease of The Ovary - Dr. TinioMonique BorresPas encore d'évaluation
- Study of Serum Creatine Phosphokinase Level in Oral Squamous Cell CarcinomaDocument4 pagesStudy of Serum Creatine Phosphokinase Level in Oral Squamous Cell CarcinomaDeepak KumarPas encore d'évaluation
- Breast Cancer 1Document29 pagesBreast Cancer 1themega1111Pas encore d'évaluation
- 2016 ESMO Essentials For Clinicians Gastrointestinal Tract Tumours (001 033)Document33 pages2016 ESMO Essentials For Clinicians Gastrointestinal Tract Tumours (001 033)Karla CbaPas encore d'évaluation
- Prostate Cancer AwarenessDocument10 pagesProstate Cancer AwarenessarthurmathieuPas encore d'évaluation
- Dentistry 07 00093Document18 pagesDentistry 07 00093Rafa LopezPas encore d'évaluation
- LIC - Cancer Cover - Brochure - 9 Inch X 8 Inch - Eng - Single PagesDocument10 pagesLIC - Cancer Cover - Brochure - 9 Inch X 8 Inch - Eng - Single PagesKumar KalyanPas encore d'évaluation
- ASCO-CAP HER2 Test Guideline Recommendations PDFDocument5 pagesASCO-CAP HER2 Test Guideline Recommendations PDFConstantinaConnieBetsiPas encore d'évaluation
- Gleason Grading SystemDocument11 pagesGleason Grading SystemElizabeth WilliamsPas encore d'évaluation
- Cancer Colon and Rectum (Wardah)Document23 pagesCancer Colon and Rectum (Wardah)WardahAliPas encore d'évaluation
- Solitary Pulmonary NoduleDocument10 pagesSolitary Pulmonary Noduleroyvillafranca100% (1)
- H-046-003250-00 CEA KIT (CLIA) Muti LaguageDocument14 pagesH-046-003250-00 CEA KIT (CLIA) Muti LaguageSinari Alfat100% (1)
- Role of Homoeopathy in The Management of LipomaDocument2 pagesRole of Homoeopathy in The Management of LipomaEditor IJTSRDPas encore d'évaluation
- Postmenopausal BleedingDocument36 pagesPostmenopausal BleedingANJU S BPas encore d'évaluation
- Sarcomas Glandula MamariaDocument6 pagesSarcomas Glandula MamariaNelly ChacónPas encore d'évaluation
- Management of Gallbladder Polyps - An Optimal Strategy ProposedDocument4 pagesManagement of Gallbladder Polyps - An Optimal Strategy ProposedTANH NGUYENPas encore d'évaluation
- Jurnal Obsos Effect of Intrauterine Copper Device On Cervical CytologyDocument20 pagesJurnal Obsos Effect of Intrauterine Copper Device On Cervical CytologySurianiPas encore d'évaluation
- Chapter 21 - The Lower Urinary Tract and Male Genital SystemDocument38 pagesChapter 21 - The Lower Urinary Tract and Male Genital SystemAgnieszka WisniewskaPas encore d'évaluation
- PIIS0031302518304471Document1 pagePIIS0031302518304471John LêPas encore d'évaluation
- London Cancer Lung Radiotherapy Guidelines 2013 v1 0Document24 pagesLondon Cancer Lung Radiotherapy Guidelines 2013 v1 0Cosmin SaftaPas encore d'évaluation
- Bowel StatisticsDocument2 pagesBowel StatisticsbillpaparounisPas encore d'évaluation
- Different Modality of Treatment For Ovarian CancerDocument2 pagesDifferent Modality of Treatment For Ovarian CancerGil LedermanPas encore d'évaluation
- LiposarkomDocument10 pagesLiposarkomAgus SusantoPas encore d'évaluation
- MCT - Patnaik Grading (1984)Document6 pagesMCT - Patnaik Grading (1984)Yurany RodriguezPas encore d'évaluation
- Pertemuan 10. Fitoterapi TumorDocument24 pagesPertemuan 10. Fitoterapi TumorDila AprianiPas encore d'évaluation
- Basic Plastic + Skin CancerDocument29 pagesBasic Plastic + Skin CancermitaPas encore d'évaluation
- Colon MediumDocument1 pageColon MediumEjak AbdillahPas encore d'évaluation
- Diagnosis and Treatment of Vulvar Precancerous Lesions and CancerDocument4 pagesDiagnosis and Treatment of Vulvar Precancerous Lesions and CancerSyahril FauziPas encore d'évaluation
- Herceptin® Trastuzumab: Albane Brunel, Claire D'avout, Domitille Fernet, Nadia TalebDocument112 pagesHerceptin® Trastuzumab: Albane Brunel, Claire D'avout, Domitille Fernet, Nadia TalebBima AnestyaPas encore d'évaluation