Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Alkylating and AntimetabolitesDocument38 pagesAlkylating and AntimetabolitesRebecca Chen0% (1)
- Oncology Drug ListDocument11 pagesOncology Drug Listashrafh100% (1)
- Chemotherapy: Chemotherapy, in Its Most General Sense, Refers To Treatment of Disease byDocument42 pagesChemotherapy: Chemotherapy, in Its Most General Sense, Refers To Treatment of Disease byMalueth AnguiPas encore d'évaluation
- NCERT Class 11 BiologyDocument345 pagesNCERT Class 11 BiologyKarthika Umashankar100% (2)
- Tamil Worksheets Class I To XDocument22 pagesTamil Worksheets Class I To Xsiva50% (4)
- Chemotherapy Protocols V 101Document42 pagesChemotherapy Protocols V 101Charm TanyaPas encore d'évaluation
- Daftar Obat Sitostatika Yang Penyimpanan Dan Pemberiannya Terlindung Dari Cahaya PDFDocument1 pageDaftar Obat Sitostatika Yang Penyimpanan Dan Pemberiannya Terlindung Dari Cahaya PDFAyahe YumnaPas encore d'évaluation
- Theodore Hong, Prajnan Das (Eds.) - Radiation Therapy For Gastrointestinal Cancers (2017, Springer InternatiDocument244 pagesTheodore Hong, Prajnan Das (Eds.) - Radiation Therapy For Gastrointestinal Cancers (2017, Springer InternatiTolga ŞanlıPas encore d'évaluation
- Body Imaging With MR & CT: 2019 Classic Lectures inDocument15 pagesBody Imaging With MR & CT: 2019 Classic Lectures insivaPas encore d'évaluation
- Apr2017Document2 pagesApr2017sivaPas encore d'évaluation
- Containment Plan For Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19)Document20 pagesContainment Plan For Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19)Vijay SharmaPas encore d'évaluation
- CRRI CircularDocument1 pageCRRI CircularsivaPas encore d'évaluation
- 4 6027044348535767490 PDFDocument1 page4 6027044348535767490 PDFsivaPas encore d'évaluation
- 4 6027044348535767490 PDFDocument1 page4 6027044348535767490 PDFsivaPas encore d'évaluation
- PDFDocument10 pagesPDFsivaPas encore d'évaluation
- 1age 2religion 3gender 4edu 5marital 10family - T11family - 14income Self - Medi MedicineDocument6 pages1age 2religion 3gender 4edu 5marital 10family - T11family - 14income Self - Medi MedicinesivaPas encore d'évaluation
- Containment Plan For Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19)Document20 pagesContainment Plan For Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19)Vijay SharmaPas encore d'évaluation
- 316 08Document9 pages316 08sivaPas encore d'évaluation
- Aim4Aiims - In: Final Mbbs Surgery McqsDocument24 pagesAim4Aiims - In: Final Mbbs Surgery McqsAnwaar YousafPas encore d'évaluation
- Rotavirus Vaccine Rates Information Sheet 0618Document10 pagesRotavirus Vaccine Rates Information Sheet 0618sivaPas encore d'évaluation
- Peak Expiratory Flow Rate Measurements Guidelines: The Royal Free Hampstead Nhs TrustDocument14 pagesPeak Expiratory Flow Rate Measurements Guidelines: The Royal Free Hampstead Nhs TrustsivaPas encore d'évaluation
- Damsbrouchre PDFDocument2 pagesDamsbrouchre PDFsivaPas encore d'évaluation
- Crackers List: (See The Pieces Atleast 15)Document1 pageCrackers List: (See The Pieces Atleast 15)sivaPas encore d'évaluation
- Studyguidev Part4 Solutions HyptestandregDocument21 pagesStudyguidev Part4 Solutions HyptestandregAmingSoejitno0% (1)
- Notes May 9, 2014 Pediatrics Part 1Document27 pagesNotes May 9, 2014 Pediatrics Part 1Diwakesh C BPas encore d'évaluation
- TN School - EMIS Student Data TemplateDocument1 pageTN School - EMIS Student Data TemplateSaravana MoorthyPas encore d'évaluation
- LicenseDocument1 pageLicenseMegatedy FredPas encore d'évaluation
- Scan0003 PDFDocument1 pageScan0003 PDFsivaPas encore d'évaluation
- M.M.SCHOOL-2016-17 - New FINAL 01.02.17Document41 pagesM.M.SCHOOL-2016-17 - New FINAL 01.02.17sivaPas encore d'évaluation
- Bacteriology Mnemonics: Corny Actors Knock Back Listerine in The Closet - The Gram Positive Bacteria Are CorynebacteriaDocument7 pagesBacteriology Mnemonics: Corny Actors Knock Back Listerine in The Closet - The Gram Positive Bacteria Are CorynebacteriahanzukikPas encore d'évaluation
- Tranexamic Acid in Gynaecology & ObstetricDocument26 pagesTranexamic Acid in Gynaecology & ObstetricsivaPas encore d'évaluation
- Studyguidev Part4 Solutions HyptestandregDocument21 pagesStudyguidev Part4 Solutions HyptestandregAmingSoejitno0% (1)
- Penetration ValueDocument13 pagesPenetration ValuesivaPas encore d'évaluation
- Standard - 4: S.No. Name Unique ID No. Class Studying Father's Name DOB Aadhaar NoDocument1 pageStandard - 4: S.No. Name Unique ID No. Class Studying Father's Name DOB Aadhaar NosivaPas encore d'évaluation
- PassportApplicationForm Main English V3.0 PDFDocument1 pagePassportApplicationForm Main English V3.0 PDFsivaPas encore d'évaluation
- Quiz Chapter 28Document23 pagesQuiz Chapter 28Amelie AvenidoPas encore d'évaluation
- 1078 Chemotherapy Extravasation Immediate Management Flow ChartDocument1 page1078 Chemotherapy Extravasation Immediate Management Flow ChartJuan Rivera VillamizarPas encore d'évaluation
- Preporuke Za Hrqol GR: Vodiči Za Karcinom ProstateDocument12 pagesPreporuke Za Hrqol GR: Vodiči Za Karcinom ProstateAndjela KosticPas encore d'évaluation
- (P3) Perhitungan Resep KemoterapiDocument28 pages(P3) Perhitungan Resep KemoterapiRESI JULIANAPas encore d'évaluation
- TARGETED THERAPY Pada Kanker ParuDocument13 pagesTARGETED THERAPY Pada Kanker Parudebby nirmasariPas encore d'évaluation
- Chemo Stability Chart - AtoKDocument59 pagesChemo Stability Chart - AtoKAfifah Nur Diana PutriPas encore d'évaluation
- 8, Identitas Pasien SoapDocument10 pages8, Identitas Pasien SoapsunarsihPas encore d'évaluation
- Anti Cancer DrugsDocument3 pagesAnti Cancer DrugsDheaPas encore d'évaluation
- Chemotherapy Sequencing Chart: Review Article Chemotherapy Administration SequenceDocument1 pageChemotherapy Sequencing Chart: Review Article Chemotherapy Administration SequencemubarakdxxPas encore d'évaluation
- Cisplatin Versus Carboplatin For Patients With Metastatic Non - Small-Cell Lung Cancer - An Old Rivalry RenewedDocument2 pagesCisplatin Versus Carboplatin For Patients With Metastatic Non - Small-Cell Lung Cancer - An Old Rivalry RenewedFlorin RizicaPas encore d'évaluation
- Minutes Prac Meeting 26 29 October 2020 - enDocument80 pagesMinutes Prac Meeting 26 29 October 2020 - enAmany HagagePas encore d'évaluation
- Bone Cancer Treatment RegimensDocument2 pagesBone Cancer Treatment RegimensAnne Lorraine BringasPas encore d'évaluation
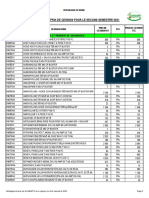
- Catalogue de Prix de Cession Pour Le Second Semestre 2021Document10 pagesCatalogue de Prix de Cession Pour Le Second Semestre 2021Mr BATTAHPas encore d'évaluation
- Role of High Dose Methotrexate in Osteosarcoma - FinalDocument30 pagesRole of High Dose Methotrexate in Osteosarcoma - FinalHemanth KumarPas encore d'évaluation
- งานเคมีบ าบัด กลุ่มงานเภสัชกรรม โรงพยาบาลราชวิถี ตาราง การเตรียมยา และความคงตัวของยาเคมีบ าบัด Reconstitution PreparationDocument11 pagesงานเคมีบ าบัด กลุ่มงานเภสัชกรรม โรงพยาบาลราชวิถี ตาราง การเตรียมยา และความคงตัวของยาเคมีบ าบัด Reconstitution Preparationtotoil22Pas encore d'évaluation
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 20Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 20EDWIN WIJAYAPas encore d'évaluation
- Trifluridine and TipiracilDocument3 pagesTrifluridine and TipiracilKristine AcasioPas encore d'évaluation
- Cancer Chemotherapy and Its ComplicationDocument49 pagesCancer Chemotherapy and Its ComplicationLina AnisaPas encore d'évaluation
- Medicamentos Antineoplásicos 27.08.2018Document6 pagesMedicamentos Antineoplásicos 27.08.2018Vagner CardosoPas encore d'évaluation
- Chemo Stability Chart LtoZDocument34 pagesChemo Stability Chart LtoZarfitaaaaPas encore d'évaluation
- Onko Iresa Fix Dr. AnaDocument48 pagesOnko Iresa Fix Dr. AnaRashya AestheticPas encore d'évaluation
- Breast Cancer ChemotherapyDocument7 pagesBreast Cancer Chemotherapydini kusmaharaniPas encore d'évaluation
- Diluent RateDocument3 pagesDiluent RateMohamed Abdel-AzizPas encore d'évaluation
- Anti - Neoplastic & ChemotherapyDocument63 pagesAnti - Neoplastic & ChemotherapyLisa JessicaPas encore d'évaluation