Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Quantitative Analysis of The Lifting Effect Of.10Document12 pagesQuantitative Analysis of The Lifting Effect Of.10Arcelino FariasPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Sarms 1 - The Ultimate Guide To SarmsDocument4 pagesSarms 1 - The Ultimate Guide To SarmsHumbert Gym ColombinaPas encore d'évaluation
- Whitepaper Psychographic SegmentationDocument32 pagesWhitepaper Psychographic SegmentationAubreyPas encore d'évaluation
- Leaflet of Bach Therapy PDFDocument2 pagesLeaflet of Bach Therapy PDFPrakash VerekarPas encore d'évaluation
- Anthelmintic DrugsDocument35 pagesAnthelmintic DrugsRamla KashifPas encore d'évaluation
- Practicing Clinical Instructor (PCI) Evaluation Form: College of NursingDocument1 pagePracticing Clinical Instructor (PCI) Evaluation Form: College of NursingJoe RealPas encore d'évaluation
- Consent Form - EmployerDocument1 pageConsent Form - EmployerShankarr Kshan100% (1)
- Compulsive Sexual Behavior PDFDocument2 pagesCompulsive Sexual Behavior PDFmaya sofianaPas encore d'évaluation
- Order Denying NHL Motion To DismissDocument33 pagesOrder Denying NHL Motion To DismissNHL Concussion LawsuitPas encore d'évaluation
- Pharma QuestionsDocument13 pagesPharma QuestionsSarah Mae SinceroPas encore d'évaluation
- Ch. 24 Older Adults Ageing in PlaceDocument54 pagesCh. 24 Older Adults Ageing in PlacebaashePas encore d'évaluation
- (Godefroy Christian) Super Health PDFDocument231 pages(Godefroy Christian) Super Health PDFAlexandre Dantas100% (1)
- Psychologist Exam With AnswersDocument13 pagesPsychologist Exam With AnswersdrashishnairPas encore d'évaluation
- Case Study Breast CancerDocument3 pagesCase Study Breast CancerJustin Joshua Derilo OrdoñaPas encore d'évaluation
- Genetic Disorders Screening and PreventionDocument36 pagesGenetic Disorders Screening and PreventionManovaPrasannaKumarPas encore d'évaluation
- Thota Act 2014Document16 pagesThota Act 2014APPas encore d'évaluation
- Chapter 41 - Thoracic Outlet Syndrome SynonymsDocument8 pagesChapter 41 - Thoracic Outlet Syndrome SynonymsPiero Massafra100% (1)
- 1 BarashDP - Paradigms Lost AbridgedDocument7 pages1 BarashDP - Paradigms Lost AbridgedFABIOPas encore d'évaluation
- 2010 Endocrine System ChartDocument3 pages2010 Endocrine System ChartAlexander QianPas encore d'évaluation
- 40 Sa Hindi - LBDocument6 pages40 Sa Hindi - LBIrshad mohammedPas encore d'évaluation
- Biochemistry and Histocytochemistry Research DevelopmentsDocument377 pagesBiochemistry and Histocytochemistry Research Developmentsfenrisulven2010100% (1)
- The Menstrual Cycle Remedies Amenorrhea HandoutDocument3 pagesThe Menstrual Cycle Remedies Amenorrhea HandoutRoger AugePas encore d'évaluation
- Beyond Schein DentalDocument9 pagesBeyond Schein DentaltomdietzlerPas encore d'évaluation
- Maverick Mark Cunningham Interview 2-14-13Document24 pagesMaverick Mark Cunningham Interview 2-14-13lublinerPas encore d'évaluation
- Moran CORE - How To Use The Direct OphthalmoscopeDocument1 pageMoran CORE - How To Use The Direct OphthalmoscopeSamsung M20APPas encore d'évaluation
- Raja Nigantu IntroductionDocument8 pagesRaja Nigantu IntroductionMedico PassPas encore d'évaluation
- High Power Electrosurgery Review Update 2005Document33 pagesHigh Power Electrosurgery Review Update 2005Ana ObradovicPas encore d'évaluation
- Contents (Continued) : Chapter 5. Nondestructive Inspection (Ndi)Document3 pagesContents (Continued) : Chapter 5. Nondestructive Inspection (Ndi)blackhawkPas encore d'évaluation
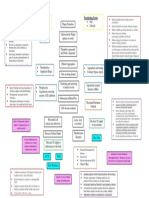
- Acute Coronary Syndrome - Concept MapDocument1 pageAcute Coronary Syndrome - Concept MapWyen CabatbatPas encore d'évaluation
- Unza Vet ReqsDocument3 pagesUnza Vet ReqsLillian Muwina100% (1)