Vous aimerez peut-être aussi
- Nursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuideD'EverandNursing: Lab Values: a QuickStudy Laminated 6-Page Reference GuidePas encore d'évaluation
- 5th Year 112 PediatricsDocument12 pages5th Year 112 PediatricsAmjad A. Amir100% (2)
- List of Drugs Approved by DCGI 1969 To Aug 2008 AlfaDocument59 pagesList of Drugs Approved by DCGI 1969 To Aug 2008 Alfagurubakkiamjai95% (19)
- Antimicrobial StewardshipDocument37 pagesAntimicrobial StewardshipsamPas encore d'évaluation
- Case Presentation On Urinary Tract InfectionDocument56 pagesCase Presentation On Urinary Tract InfectionJohn Alvin Yoro92% (24)
- CPT Coding Practice QuestionsDocument10 pagesCPT Coding Practice QuestionsTannu SamadPas encore d'évaluation
- Hospital Quality IndicatorsDocument32 pagesHospital Quality Indicatorsakhtarulmunim2279Pas encore d'évaluation
- Hospital Antibiotic PolicyDocument5 pagesHospital Antibiotic PolicyNaveen ArichwalPas encore d'évaluation
- Morning Report Case: MarchDocument20 pagesMorning Report Case: Marchputri meiliawatiPas encore d'évaluation
- Morning Report Case: 16th July, 2012Document18 pagesMorning Report Case: 16th July, 2012Felicia adeline ChristianPas encore d'évaluation
- Morning Report: Thursday, November 15 2018Document21 pagesMorning Report: Thursday, November 15 2018Lipo DuoPas encore d'évaluation
- Morning Report Case: June 19, 2014Document23 pagesMorning Report Case: June 19, 2014Sri DashiniePas encore d'évaluation
- Morning ReportDocument17 pagesMorning ReportBanng BinggPas encore d'évaluation
- MR 5 November 2018Document16 pagesMR 5 November 2018BakingpancakesPas encore d'évaluation
- Morning Report Case: June 7, 2011Document16 pagesMorning Report Case: June 7, 2011LittleChenaPas encore d'évaluation
- MR SipDocument26 pagesMR SipFelicia adeline ChristianPas encore d'évaluation
- MR IleusDocument24 pagesMR IleusFelicia adeline ChristianPas encore d'évaluation
- Morning Report: 7 February 2011Document20 pagesMorning Report: 7 February 2011adi_ancuxPas encore d'évaluation
- Morning Report: Sunday, Oktober 7 2018Document21 pagesMorning Report: Sunday, Oktober 7 2018Bhisma DewabrathaPas encore d'évaluation
- Afternoon Report 9 April 2017Document17 pagesAfternoon Report 9 April 2017Puteri Diah RahtiniPas encore d'évaluation
- Morning Report Case: 16th July, 2012Document20 pagesMorning Report Case: 16th July, 2012Felicia adeline ChristianPas encore d'évaluation
- MR Dhiarrea 10 September 2018Document17 pagesMR Dhiarrea 10 September 2018GustiAyuNindyaPas encore d'évaluation
- Ar Anemia Aplastik SherylDocument42 pagesAr Anemia Aplastik SherylSheryl ElitaPas encore d'évaluation
- MR GoutyDocument25 pagesMR GoutyArvindan SubramaniamPas encore d'évaluation
- Duty Report Saturday, May 2 2015 Dr. Ramadhan Physician in ChargeDocument6 pagesDuty Report Saturday, May 2 2015 Dr. Ramadhan Physician in ChargeCristian RajagukgukPas encore d'évaluation
- Morning Report: Dr. Dikara WS Maulidy, SP - PDDocument24 pagesMorning Report: Dr. Dikara WS Maulidy, SP - PDBethari Abi SafitriPas encore d'évaluation
- Contoh Morning ReportDocument23 pagesContoh Morning ReportDaondy Friarsa SoehartoPas encore d'évaluation
- MR Belakang 24022021 RAM Ca Buli EDITDocument25 pagesMR Belakang 24022021 RAM Ca Buli EDITWilujeng AnggrainiPas encore d'évaluation
- MR DR - Yusra, SP - JP 16 Sept 2020Document30 pagesMR DR - Yusra, SP - JP 16 Sept 2020Feny Niifeny 'mcqueen'Pas encore d'évaluation
- Morning Report: Friday 20 April 2012Document18 pagesMorning Report: Friday 20 April 2012Felicia adeline ChristianPas encore d'évaluation
- LeptospirosisDocument19 pagesLeptospirosisFelicia adeline ChristianPas encore d'évaluation
- FINAL CervicalCA7BDocument6 pagesFINAL CervicalCA7BRommel OliverasPas encore d'évaluation
- Morning Report Case: Desember 15 TH 2016Document15 pagesMorning Report Case: Desember 15 TH 2016Pramana AdiputraPas encore d'évaluation
- Acute Limfoid Leukemia: Morning Report April 10 2015Document22 pagesAcute Limfoid Leukemia: Morning Report April 10 2015Diah Rahayu100% (1)
- Morning Report Case: 18th July, 2012Document19 pagesMorning Report Case: 18th July, 2012Felicia adeline ChristianPas encore d'évaluation
- Morning Case Report: August 9th, 2014Document23 pagesMorning Case Report: August 9th, 2014hragunathanPas encore d'évaluation
- Case Report COPDDocument18 pagesCase Report COPDMia RisdayanthiPas encore d'évaluation
- POMR FIN CholangitisDocument29 pagesPOMR FIN Cholangitisphyna27Pas encore d'évaluation
- Morning Case Report January 3, 2016Document15 pagesMorning Case Report January 3, 2016Pradnya ParamithaPas encore d'évaluation
- Hypocalcemia, Hypoparathyroid WahyuDocument27 pagesHypocalcemia, Hypoparathyroid WahyuFerdinando BaehaPas encore d'évaluation
- NC - Muhammad RaditDocument18 pagesNC - Muhammad RaditDodi DiPas encore d'évaluation
- SOS AYU - Ax - PeunjangDocument11 pagesSOS AYU - Ax - PeunjangIka AyuPas encore d'évaluation
- Duty Report Chronic Kidney Diseases, DM and GERD: Approach of Complexity ProblemDocument15 pagesDuty Report Chronic Kidney Diseases, DM and GERD: Approach of Complexity ProblemGiovina FajarPas encore d'évaluation
- MR 190820 Dr. Haudhiya OkeDocument53 pagesMR 190820 Dr. Haudhiya OkeRudy Arindra WijayaPas encore d'évaluation
- Heteroanamnesa Chief Complaint: Coffe Ground Vomiting History of Present IllnessDocument6 pagesHeteroanamnesa Chief Complaint: Coffe Ground Vomiting History of Present IllnessIka AyuPas encore d'évaluation
- Morning ReportDocument27 pagesMorning ReportDody PrasetyaPas encore d'évaluation
- Bab Ii Laporan Kasus: 2.1 IdentifikasiDocument13 pagesBab Ii Laporan Kasus: 2.1 IdentifikasiRikka Wijaya JfPas encore d'évaluation
- Case Presentation On Chronic Liver Disease: Shreyas M Salimath Pharm D 2 Year REG NO. 21Q0172Document18 pagesCase Presentation On Chronic Liver Disease: Shreyas M Salimath Pharm D 2 Year REG NO. 21Q0172AmalinPas encore d'évaluation
- Crypt Orchid Is MDocument29 pagesCrypt Orchid Is Mzackypradana95Pas encore d'évaluation
- MR Placenta Previa Dr. Edy SpOGDocument17 pagesMR Placenta Previa Dr. Edy SpOGtiaraPas encore d'évaluation
- Asma Bronkiale: Pembimbing: Prof. Dr. Dr. Tjok Raka Putra, SPPD-KRDocument8 pagesAsma Bronkiale: Pembimbing: Prof. Dr. Dr. Tjok Raka Putra, SPPD-KRGustiAyuNindyaPas encore d'évaluation
- Case Report Prolaps UteriDocument21 pagesCase Report Prolaps UteriRiris RaudyaPas encore d'évaluation
- Morning Report Case: 24 April, 2012Document20 pagesMorning Report Case: 24 April, 2012Renata YolandaPas encore d'évaluation
- Case Based DiscussionDocument49 pagesCase Based DiscussionMaulana IbrahimPas encore d'évaluation
- Case Report Case ReportDocument18 pagesCase Report Case ReportMelly MirandaPas encore d'évaluation
- Morning Report: Date: 6 April 2021Document17 pagesMorning Report: Date: 6 April 2021Adinda DianPas encore d'évaluation
- POMR 3 - Ogie Efusi PleuraDocument16 pagesPOMR 3 - Ogie Efusi PleurahariogiePas encore d'évaluation
- Mrs. Fera Febriyani/ 27 y.o/MR 1.43.51.17 Admitted On July 27 2019 at 11.00 PMDocument11 pagesMrs. Fera Febriyani/ 27 y.o/MR 1.43.51.17 Admitted On July 27 2019 at 11.00 PMmonyet65Pas encore d'évaluation
- Ahmad Basori VidiDocument30 pagesAhmad Basori VidiIka AyuPas encore d'évaluation
- Latihan POMR: Dr. Venna Febrian KDocument39 pagesLatihan POMR: Dr. Venna Febrian KLoudry ElfaPas encore d'évaluation
- NC FARHAN RESPI SalinanDocument21 pagesNC FARHAN RESPI SalinanRima KhairunnisaPas encore d'évaluation
- Morning Report: June 2022 Physician in ChargeDocument24 pagesMorning Report: June 2022 Physician in ChargeIka AyuPas encore d'évaluation
- Nanda Hematemesis MelenaDocument13 pagesNanda Hematemesis MelenaLiya AnjelinaPas encore d'évaluation
- POMR 9 Pseudo Meigs Syndrome - OgieDocument21 pagesPOMR 9 Pseudo Meigs Syndrome - OgiehariogiePas encore d'évaluation
- Morning ReportDocument22 pagesMorning ReportNiinna AwliaPas encore d'évaluation
- Infective EndocarditisDocument8 pagesInfective EndocarditisAiman Arifin100% (1)
- Morning Report Case: June 18th, 2012Document13 pagesMorning Report Case: June 18th, 2012Felicia adeline ChristianPas encore d'évaluation
- Morning Case Report: October 4th 2011Document22 pagesMorning Case Report: October 4th 2011Felicia adeline ChristianPas encore d'évaluation
- Morning Report Case: June 18th, 2012Document13 pagesMorning Report Case: June 18th, 2012Felicia adeline ChristianPas encore d'évaluation
- Morning Report Case: Februari 19, 2010Document17 pagesMorning Report Case: Februari 19, 2010Felicia adeline ChristianPas encore d'évaluation
- COPD + Acute ExacerbationDocument23 pagesCOPD + Acute ExacerbationFelicia adeline ChristianPas encore d'évaluation
- Morning Report: Friday 20 April 2012Document18 pagesMorning Report: Friday 20 April 2012Felicia adeline ChristianPas encore d'évaluation
- MR AnafilaksisDocument23 pagesMR AnafilaksisFelicia adeline ChristianPas encore d'évaluation
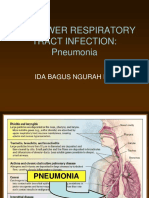
- The Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiDocument32 pagesThe Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiFelicia adeline ChristianPas encore d'évaluation
- Morning Report Case: 18th July, 2012Document19 pagesMorning Report Case: 18th July, 2012Felicia adeline ChristianPas encore d'évaluation
- MR IleusDocument24 pagesMR IleusFelicia adeline ChristianPas encore d'évaluation
- Morning Report Case: 16th July, 2012Document20 pagesMorning Report Case: 16th July, 2012Felicia adeline ChristianPas encore d'évaluation
- MR SipDocument26 pagesMR SipFelicia adeline ChristianPas encore d'évaluation
- MR AnafilaksisDocument23 pagesMR AnafilaksisFelicia adeline ChristianPas encore d'évaluation
- Morning Report Case: October 27 2010Document33 pagesMorning Report Case: October 27 2010Felicia adeline ChristianPas encore d'évaluation
- LeptospirosisDocument19 pagesLeptospirosisFelicia adeline ChristianPas encore d'évaluation
- COPD + Acute ExacerbationDocument23 pagesCOPD + Acute ExacerbationFelicia adeline ChristianPas encore d'évaluation
- Morning Report Case: June 18th, 2012Document13 pagesMorning Report Case: June 18th, 2012Felicia adeline ChristianPas encore d'évaluation
- Morning Report Case: Februari 19, 2010Document17 pagesMorning Report Case: Februari 19, 2010Felicia adeline ChristianPas encore d'évaluation
- The Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiDocument32 pagesThe Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiFelicia adeline ChristianPas encore d'évaluation
- Textbook ReadingDocument42 pagesTextbook ReadingFelicia adeline ChristianPas encore d'évaluation
- Journal ReadingDocument13 pagesJournal ReadingFelicia adeline ChristianPas encore d'évaluation
- Chlamydia GonorrheaDocument3 pagesChlamydia GonorrheaAugene ToribioPas encore d'évaluation
- Urology: Magazine For Companion-Animal PractitionersDocument48 pagesUrology: Magazine For Companion-Animal PractitionersJuan Carlos Ortiz RamirezPas encore d'évaluation
- Case Study P.TDocument5 pagesCase Study P.TSharon WilliamsPas encore d'évaluation
- FNCP UTIDocument2 pagesFNCP UTITel EscorialPas encore d'évaluation
- Acute PyelonephritisDocument9 pagesAcute Pyelonephritistaekado-1Pas encore d'évaluation
- Urinary Tract InfectionDocument7 pagesUrinary Tract InfectionCaressie BiscoPas encore d'évaluation
- Savina Madliena JurnalDocument6 pagesSavina Madliena JurnalTaufan Putra WidodoPas encore d'évaluation
- Dr. Paksi-BPH Paksi BandungDocument53 pagesDr. Paksi-BPH Paksi BandungradenayulistyaPas encore d'évaluation
- Urinary and Male GenitalDocument116 pagesUrinary and Male GenitalMultazam ZamPas encore d'évaluation
- Acute Uncomplicated PyelonephritisDocument5 pagesAcute Uncomplicated PyelonephritisoreaPas encore d'évaluation
- Urinary Tract AntisepticDocument14 pagesUrinary Tract AntisepticAnson Marokey100% (1)
- Intensive Care Units Role of NursingDocument69 pagesIntensive Care Units Role of Nursingtummalapalli venkateswara raoPas encore d'évaluation
- Antimicrobial Screening of Staphylococcus Aureus in Different Clinical Specimen of Urine in DuhaiDocument13 pagesAntimicrobial Screening of Staphylococcus Aureus in Different Clinical Specimen of Urine in DuhaiIJRASETPublicationsPas encore d'évaluation
- NMJ VOL5 NO2 Final 44 49Document6 pagesNMJ VOL5 NO2 Final 44 49Ravi GuptaPas encore d'évaluation
- Chapter 2 - Formulating An Effective Response - A Structured ApproachDocument20 pagesChapter 2 - Formulating An Effective Response - A Structured Approachreham OPas encore d'évaluation
- Olainfarm Product CatalogueDocument40 pagesOlainfarm Product Catalogueeverstrong0% (1)
- Two Chinese Food Therapies To Prevent UTIDocument2 pagesTwo Chinese Food Therapies To Prevent UTIvivianPas encore d'évaluation
- CH 20 Nursing Care of A Family Experiencing A Pregnancy ComplicationDocument18 pagesCH 20 Nursing Care of A Family Experiencing A Pregnancy Complicationcutiepie creampiePas encore d'évaluation
- UTI MCQDocument10 pagesUTI MCQHomman TommanPas encore d'évaluation
- Vet Pharm ReportDocument4 pagesVet Pharm ReportTusvendran PillaiPas encore d'évaluation
- Infectious Causes of Dysuria in Adult MenDocument5 pagesInfectious Causes of Dysuria in Adult MenFrancisco Javier Contreras MoralesPas encore d'évaluation
- IM - UTI Harrison's Personal NotesDocument5 pagesIM - UTI Harrison's Personal NotesstoragejoannamsvPas encore d'évaluation
- Students Individual Teaching PlanDocument2 pagesStudents Individual Teaching PlanNOEL YRIGONPas encore d'évaluation