Vous aimerez peut-être aussi
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingD'EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováPas encore d'évaluation
- Problem-based Approach to Gastroenterology and HepatologyD'EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisPas encore d'évaluation
- ComaDocument13 pagesComaMamoon J. MehdiPas encore d'évaluation
- Emergency Management of DKADocument12 pagesEmergency Management of DKAtinzioPas encore d'évaluation
- PneumoniaDocument48 pagesPneumoniaSiti FatimahPas encore d'évaluation
- Community Acquired PneumoniaDocument37 pagesCommunity Acquired PneumoniaJoean CabarlocPas encore d'évaluation
- Diverticular Disease of The ColonDocument38 pagesDiverticular Disease of The Colonapi-19641337Pas encore d'évaluation
- ClubbingDocument44 pagesClubbingAkshat Srivastava100% (1)
- Pneumonia and Lung AbscessDocument50 pagesPneumonia and Lung AbscessMarc Imhotep Cray, M.D.Pas encore d'évaluation
- HyperglycemiaDocument1 pageHyperglycemiaanon_262360776Pas encore d'évaluation
- GP Reg - Asthma and Spirometry 2011Document114 pagesGP Reg - Asthma and Spirometry 2011minerva_stanciuPas encore d'évaluation
- Tratament PneumonieDocument32 pagesTratament PneumonieSerban Elena100% (1)
- COPD Causes, Risk Factors, and Natural HistoryDocument45 pagesCOPD Causes, Risk Factors, and Natural HistoryNogra CarlPas encore d'évaluation
- Pathophysiology of AsthmaDocument71 pagesPathophysiology of AsthmaChin ChanPas encore d'évaluation
- DR Anuj Raj BijukchheDocument95 pagesDR Anuj Raj BijukchheMUHAMMAD JAWAD HASSANPas encore d'évaluation
- Upper Gi BleedingDocument3 pagesUpper Gi BleedingIkhwan HafrizPas encore d'évaluation
- Fungal Ear Infection & Scalp Ringworm GuideDocument7 pagesFungal Ear Infection & Scalp Ringworm GuideFaiq LPas encore d'évaluation
- Instant Alert For Myocardial Infarction Keshav Singhal Shri Vaishnav Institute of Tech. & Science Indore EMAIL ADD: Keshav - Svits@yahoo - Co.inDocument7 pagesInstant Alert For Myocardial Infarction Keshav Singhal Shri Vaishnav Institute of Tech. & Science Indore EMAIL ADD: Keshav - Svits@yahoo - Co.inKeshav SinghalPas encore d'évaluation
- Pneumonia: Prepared By: Leila Rose D. Sanson BSN - 2CDocument7 pagesPneumonia: Prepared By: Leila Rose D. Sanson BSN - 2CDoc DudayPas encore d'évaluation
- 2020 International Society of Hypertension Global Hypertension Practice GuidelinesDocument48 pages2020 International Society of Hypertension Global Hypertension Practice GuidelinesNicoleta Popa-FoteaPas encore d'évaluation
- Pathophysiology Respiratory SystemDocument63 pagesPathophysiology Respiratory SystemAli Basha QudahPas encore d'évaluation
- Bronchial AsthmaDocument54 pagesBronchial AsthmaSehar162100% (2)
- Copd 200412082048Document139 pagesCopd 200412082048Richard ArcePas encore d'évaluation
- Pulmonary ThromboembolismDocument61 pagesPulmonary ThromboembolismsanjivdasPas encore d'évaluation
- Optimized Clinical Case StudiesDocument4 pagesOptimized Clinical Case StudiesAassh DcmbrPas encore d'évaluation
- Pneumonia: Submitted To:Ms Lisette Cruz Submitted By: Ms. Mely Rose AbanadorDocument26 pagesPneumonia: Submitted To:Ms Lisette Cruz Submitted By: Ms. Mely Rose AbanadorJoyce Catherine Buquing UysecoPas encore d'évaluation
- Surgery Case AppendicitisDocument30 pagesSurgery Case AppendicitisSarahPas encore d'évaluation
- Pathology of The Lung: Djumadi AchmadDocument26 pagesPathology of The Lung: Djumadi AchmadVivi DeviyanaPas encore d'évaluation
- Depression: Understanding the Leading Mental Health ConditionDocument38 pagesDepression: Understanding the Leading Mental Health Conditiondrmsupriya091159Pas encore d'évaluation
- Cardiovascular System: by DR - Nuha Abdel GhaffarDocument41 pagesCardiovascular System: by DR - Nuha Abdel GhaffarMohammed Alaa EldeanPas encore d'évaluation
- Langerhans Cell HistiocytosisDocument7 pagesLangerhans Cell HistiocytosisDarwin ElguiraPas encore d'évaluation
- Introduction Diabetic MellitusDocument3 pagesIntroduction Diabetic MellitusharpreetsainiPas encore d'évaluation
- RBC Degradation & Causes of JaundiceDocument30 pagesRBC Degradation & Causes of JaundiceSubhi MishraPas encore d'évaluation
- Type 2 Diabetes Mellitus and Chronic ComplicationsDocument6 pagesType 2 Diabetes Mellitus and Chronic ComplicationsInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Sweet Syndrome EnglishDocument19 pagesSweet Syndrome EnglishAsma AlwiPas encore d'évaluation
- Guide to Diagnosing and Treating PneumoniaDocument67 pagesGuide to Diagnosing and Treating PneumoniaManisanthosh Kumar100% (1)
- Case Presentation On Recurrent PULMONARY EMBOLISMDocument14 pagesCase Presentation On Recurrent PULMONARY EMBOLISMAkas RehmanPas encore d'évaluation
- Approach To Patients With LymphadenopathyDocument5 pagesApproach To Patients With LymphadenopathyAngela Mitchelle NyanganPas encore d'évaluation
- Diagnosis of Portal Hypertension 1Document20 pagesDiagnosis of Portal Hypertension 1sussie jeffersonPas encore d'évaluation
- Heart AttackDocument2 pagesHeart Attackmeylisa putri ayunandaPas encore d'évaluation
- The Pneumonias: Types, Causes, Symptoms and TreatmentsDocument60 pagesThe Pneumonias: Types, Causes, Symptoms and TreatmentsCristina Georgiana CoticăPas encore d'évaluation
- Liver Cirrhosis (VD)Document56 pagesLiver Cirrhosis (VD)HannaTashiaClaudiaPas encore d'évaluation
- Epiglottitis PDFDocument5 pagesEpiglottitis PDFhasan benokriPas encore d'évaluation
- Asthma Pathophysiology and Risk FactorsDocument98 pagesAsthma Pathophysiology and Risk FactorsyayayanizaPas encore d'évaluation
- Lower GI Bleeding Causes and Treatment OptionsDocument42 pagesLower GI Bleeding Causes and Treatment OptionsRaja Ain100% (1)
- Dilated CardiomyopathyDocument27 pagesDilated CardiomyopathyPaula Vanessa RN100% (1)
- Sputum ExamDocument14 pagesSputum ExamJuan MorsePas encore d'évaluation
- AnswersDocument47 pagesAnswersOriyomi OdekunlePas encore d'évaluation
- Lung AbscessDocument27 pagesLung AbscessMalueth Angui100% (1)
- ScabiesDocument15 pagesScabiesAbdullah Mascardo BarabagPas encore d'évaluation
- Asthma Patient ProfileDocument8 pagesAsthma Patient ProfileGlenn Asuncion PagaduanPas encore d'évaluation
- Diagnosing Chest Pain CausesDocument8 pagesDiagnosing Chest Pain CausesMedisina101Pas encore d'évaluation
- Adrenal DisordersDocument29 pagesAdrenal DisordersSuliman Garalleh100% (1)
- Module 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - ClementeDocument27 pagesModule 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - Clementeelaine100% (1)
- MOSCO'S CLERKING GUIDEDocument88 pagesMOSCO'S CLERKING GUIDEtemitopePas encore d'évaluation
- Bronchial Asthma and Acute AsthmaDocument38 pagesBronchial Asthma and Acute AsthmaFreddy KassimPas encore d'évaluation
- PLEURAL EFFUSION CAUSES AND DIAGNOSISDocument52 pagesPLEURAL EFFUSION CAUSES AND DIAGNOSISvaishnaviPas encore d'évaluation
- AsthmaDocument39 pagesAsthmamits98Pas encore d'évaluation
- Approach To The Patient With Cough and Hemoptysis 15 11 13Document34 pagesApproach To The Patient With Cough and Hemoptysis 15 11 13Sanchit PeriwalPas encore d'évaluation
- Clinical Pharmacology: Proceedings of the 7th International Congress of Pharmacology, Paris 1978D'EverandClinical Pharmacology: Proceedings of the 7th International Congress of Pharmacology, Paris 1978P. Duchêne-MarullazPas encore d'évaluation
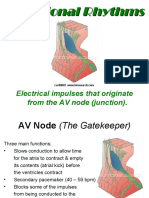
- Irama JunctionalDocument18 pagesIrama JunctionalTaufik Nur YahyaPas encore d'évaluation
- Rekonstruksi VaskularDocument33 pagesRekonstruksi VaskularTaufik Nur YahyaPas encore d'évaluation
- Chest Tube Insertion GuideDocument8 pagesChest Tube Insertion GuideTaufik Nur YahyaPas encore d'évaluation
- Antibacterial DrugsDocument56 pagesAntibacterial DrugsTaufik Nur Yahya100% (1)
- Pneumonia: Nur Yahya, T 05/1087561/KU/11522Document19 pagesPneumonia: Nur Yahya, T 05/1087561/KU/11522Taufik Nur YahyaPas encore d'évaluation
- NTU VirusBom EngDocument51 pagesNTU VirusBom EngdavincegigaPas encore d'évaluation
- Risk For AspirationDocument2 pagesRisk For AspirationGly Mtg100% (6)
- COVID Health Screening FormDocument2 pagesCOVID Health Screening FormJohnna Pauline VirayPas encore d'évaluation
- CME - Breathlessness RadDocument51 pagesCME - Breathlessness Radjun sianPas encore d'évaluation
- Daftar PustakaDocument6 pagesDaftar PustakaphineeeeePas encore d'évaluation
- Covid-19 SpeechDocument2 pagesCovid-19 SpeechNur IlaynaPas encore d'évaluation
- Routine Immunization - Details - For 4th August MetingDocument57 pagesRoutine Immunization - Details - For 4th August Metingjalanayush777Pas encore d'évaluation
- Lung AbscessDocument26 pagesLung AbscessPrajwal Rao KPas encore d'évaluation
- COVID-19 Prevention TipsDocument4 pagesCOVID-19 Prevention TipsBeti SimunPas encore d'évaluation
- Annotated BibliographyDocument6 pagesAnnotated BibliographyStanley PierrePas encore d'évaluation
- Asthma Action PlanDocument2 pagesAsthma Action PlanQuan DinhPas encore d'évaluation
- IM Concept Map SGD Group 13, Fever and CoughDocument4 pagesIM Concept Map SGD Group 13, Fever and Coughb8gjhmq6rrPas encore d'évaluation
- Respiratory MCQs LJDocument7 pagesRespiratory MCQs LJfjghPas encore d'évaluation
- Occupational Lung DiseaseDocument24 pagesOccupational Lung DiseaseprachitiPas encore d'évaluation
- Path Lung McqsDocument24 pagesPath Lung McqsShafaque IrfanPas encore d'évaluation
- How Long Does A Cough Normally Last?Document4 pagesHow Long Does A Cough Normally Last?Dalveer JohnPas encore d'évaluation
- Imaging and HRCT Chest in Covid-19Document42 pagesImaging and HRCT Chest in Covid-19Siti Kembang100% (1)
- Bronchiectasis: Definition: Prognosis & ProgressionDocument1 pageBronchiectasis: Definition: Prognosis & ProgressionMohammad AbbasPas encore d'évaluation
- Astm Curs Stud 22-23Document44 pagesAstm Curs Stud 22-23Irina ASPas encore d'évaluation
- English Conversation Discussion About AllergiesDocument3 pagesEnglish Conversation Discussion About AllergiesKevin ScottPas encore d'évaluation
- Pulmonology: The Cells of The Bronchial Epithelium, LeucocytesDocument64 pagesPulmonology: The Cells of The Bronchial Epithelium, LeucocytesSk Chaudhry100% (1)
- Manuskrip KTI ZikriDocument13 pagesManuskrip KTI ZikriZikri NurhidayatPas encore d'évaluation
- Health Teaching Plan For Cough and ColdDocument10 pagesHealth Teaching Plan For Cough and ColdMae VisperasPas encore d'évaluation
- Hao Medical Clnic Family Medicine: Buhangin, Davao CityDocument2 pagesHao Medical Clnic Family Medicine: Buhangin, Davao CityJulie Ann LacandulaPas encore d'évaluation
- Daftar Diagnosa Penyakit Berdasarkan Icd-10: Poli Dalam Poli ParuDocument4 pagesDaftar Diagnosa Penyakit Berdasarkan Icd-10: Poli Dalam Poli ParuNannda SuccindaaPas encore d'évaluation
- Influenza Virus & Parainfluenza Virus - EnglishDocument17 pagesInfluenza Virus & Parainfluenza Virus - EnglishEmanuelWayan100% (1)
- 4-Larynx. Cong&trauma of LarynxDocument26 pages4-Larynx. Cong&trauma of LarynxislamPas encore d'évaluation
- Https Testservices - Nic.in ExamSys21 DownloadAdmitCard AdmitCardCTETPre - AspxDocument1 pageHttps Testservices - Nic.in ExamSys21 DownloadAdmitCard AdmitCardCTETPre - AspxAkleshwar CoolPas encore d'évaluation
- Self-Disclosure by Contractor Employees COVID-19 (English)Document1 pageSelf-Disclosure by Contractor Employees COVID-19 (English)peters petersPas encore d'évaluation
- Cebu Institute of Technology - University: Nursing Care PlanDocument2 pagesCebu Institute of Technology - University: Nursing Care PlanSergiPas encore d'évaluation