Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- L5R Traps 5e (Donjon Translation)Document1 pageL5R Traps 5e (Donjon Translation)Jose Manuel Caeiro TopaPas encore d'évaluation
- Manual Pivot ShuttleDocument18 pagesManual Pivot ShuttleFidel OrtizPas encore d'évaluation
- 4AT Automatic TransDocument126 pages4AT Automatic TransdrPas encore d'évaluation
- Syh 1552 PDFDocument1 pageSyh 1552 PDFSella Pegaso PegasoPas encore d'évaluation
- Safety Life at SeaDocument12 pagesSafety Life at SeataufikppnsPas encore d'évaluation
- Emirates A380 PDFDocument1 pageEmirates A380 PDFNur TangkianPas encore d'évaluation
- Learning Activity 3: Fuente: SENADocument3 pagesLearning Activity 3: Fuente: SENAjairo andres vargas ruedaPas encore d'évaluation
- Muscle Strengthening ExerciseDocument15 pagesMuscle Strengthening ExerciseLorencePas encore d'évaluation
- Wheel AlignmentDocument4 pagesWheel AlignmentdonlynPas encore d'évaluation
- Champ Handbook v1 Amtgard WestmarchDocument40 pagesChamp Handbook v1 Amtgard WestmarchLacey ArvinPas encore d'évaluation
- D&D Character Sheet 18Document3 pagesD&D Character Sheet 18greta ubermenschPas encore d'évaluation
- Staff No Name Stat Station GradeDocument40 pagesStaff No Name Stat Station Graderadhey shyam sharmaPas encore d'évaluation
- Ford Reg Epc PDFDocument4 pagesFord Reg Epc PDFHumberto LojanPas encore d'évaluation
- Anatomy of Pain Trigger Point Therapy For Exercise Professionals Exam Pack 0616Document42 pagesAnatomy of Pain Trigger Point Therapy For Exercise Professionals Exam Pack 0616Dharmender Singh67% (3)
- 2012-05-12 12.50.32 ErrorDocument12 pages2012-05-12 12.50.32 ErrorHori TaizoPas encore d'évaluation
- Mens Health October 2016 UK PDFDocument226 pagesMens Health October 2016 UK PDFAj YangPas encore d'évaluation
- Resistance TrainingDocument4 pagesResistance TrainingRuchelle Denice Demaisip IIPas encore d'évaluation
- Star Wars d20 - Ultimate Alien AnthologyDocument229 pagesStar Wars d20 - Ultimate Alien Anthologyannabella4497% (37)
- Elan Skis Racing Catalogue 1314 PDFDocument7 pagesElan Skis Racing Catalogue 1314 PDFwest werbeagenturPas encore d'évaluation
- Saucy Skimmer AKA Saucy Shingle Hydroplane Boat PlansDocument8 pagesSaucy Skimmer AKA Saucy Shingle Hydroplane Boat PlansJim100% (6)
- CMC ST 350: Compost TurnerDocument2 pagesCMC ST 350: Compost TurnerCarlosPas encore d'évaluation
- 1/2LH - PE Report Comments - Semester 1, 2020 - Tracey KennedyDocument2 pages1/2LH - PE Report Comments - Semester 1, 2020 - Tracey Kennedytracey kennedyPas encore d'évaluation
- Easy EKGDocument45 pagesEasy EKGnov14Pas encore d'évaluation
- K. Gábor: Koffol's Sample Training Program Hypertrophy - Week 2Document2 pagesK. Gábor: Koffol's Sample Training Program Hypertrophy - Week 2Koffi GáborPas encore d'évaluation
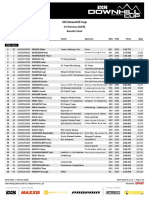
- Results Finals DHC #4 Ilmenau 2023Document12 pagesResults Finals DHC #4 Ilmenau 2023racementPas encore d'évaluation
- Balance Bar Design and Motion Analysis of Pushrod: Research PaperDocument4 pagesBalance Bar Design and Motion Analysis of Pushrod: Research PaperParas kapoorPas encore d'évaluation
- Fsu Feather - Google SearchDocument1 pageFsu Feather - Google SearchSophia RyanPas encore d'évaluation
- DL650K9Document187 pagesDL650K9Juan Abraham AjpopPas encore d'évaluation
- Chapter 01 (Intro)Document14 pagesChapter 01 (Intro)Hajim Amir SallehPas encore d'évaluation