Vous aimerez peut-être aussi
- Rancang Bangun Alat Hypo-Hyperthermia Berbasis ArduinoDocument8 pagesRancang Bangun Alat Hypo-Hyperthermia Berbasis ArduinoRAHMAT BAHTIARBPas encore d'évaluation
- Prinsip Kerja Patient Monitor PDFDocument3 pagesPrinsip Kerja Patient Monitor PDFHafid Sang PemimpiPas encore d'évaluation
- Struma Nodulus Non ToksikDocument32 pagesStruma Nodulus Non Toksikderahmat dedyPas encore d'évaluation
- SOP SpektrofotometerDocument2 pagesSOP SpektrofotometerTami EeiroutaPas encore d'évaluation
- Sop Suction PumpDocument2 pagesSop Suction PumpNila WatiPas encore d'évaluation
- Awake Versus Deep ExtubationDocument22 pagesAwake Versus Deep Extubationtipanan_earnPas encore d'évaluation
- Indikator Saturasi OksigenDocument1 pageIndikator Saturasi OksigenAulinaPas encore d'évaluation
- Refrat Obat Anestesi RilaDocument69 pagesRefrat Obat Anestesi RilaRila RivandaPas encore d'évaluation
- Daftar Nutrisi ParenteralDocument6 pagesDaftar Nutrisi Parenteralcitrahdyn100% (1)
- Jurnal Hipotermi Cairan PenghangatDocument6 pagesJurnal Hipotermi Cairan PenghangatcahyaPas encore d'évaluation
- Kebutuhan Alat Alat AnestesiDocument5 pagesKebutuhan Alat Alat AnestesiidrisPas encore d'évaluation
- Biodata Parestesi Juli 2011 Edit IpoDocument56 pagesBiodata Parestesi Juli 2011 Edit Iporahmat feryadiPas encore d'évaluation
- PEDOMAN Tatalaksana Cedera Otak 2014Document96 pagesPEDOMAN Tatalaksana Cedera Otak 2014hasanPas encore d'évaluation
- Biphasic DefbrillationDocument16 pagesBiphasic DefbrillationchanlalPas encore d'évaluation
- Leprosy: Pathogenesis Updated: ReviewDocument15 pagesLeprosy: Pathogenesis Updated: ReviewagneselimPas encore d'évaluation
- Monitoring Neuromuskular Kuantitatif Pada Penggunaan Muscle RelaxantDocument17 pagesMonitoring Neuromuskular Kuantitatif Pada Penggunaan Muscle RelaxantWidi Yuli HariantoPas encore d'évaluation
- Edema ParuDocument42 pagesEdema ParuGP RS EMCPas encore d'évaluation
- Cairan CaseDocument7 pagesCairan CaseBryan HoriandoPas encore d'évaluation
- TE332 e PDFDocument2 pagesTE332 e PDFPhat Lu AnhPas encore d'évaluation
- Spesifikasi PHILIPS Ultrasound System EPIQ 5 WHC BasicDocument2 pagesSpesifikasi PHILIPS Ultrasound System EPIQ 5 WHC BasichsPas encore d'évaluation
- Taping OA Genu Dr. SIsca Susantio, Sp. KFRDocument11 pagesTaping OA Genu Dr. SIsca Susantio, Sp. KFRDsk IndryPas encore d'évaluation
- Anatomi Dan Fisiologi TidurDocument25 pagesAnatomi Dan Fisiologi TidurMuhammad HidayatPas encore d'évaluation
- Tatalaksana ACS HUT Harkit 2015Document35 pagesTatalaksana ACS HUT Harkit 2015Muhammad Jahari SupiantoPas encore d'évaluation
- Ranking Unas SmakDocument14 pagesRanking Unas Smakl0stsga123Pas encore d'évaluation
- Kuliah Dermato Terapi 2013Document46 pagesKuliah Dermato Terapi 2013Vania EssiandaPas encore d'évaluation
- Monitoring Intra Operatif: Mindi Widayani NRP 122.022.1115 FK UPN "Veteran" JakartaDocument21 pagesMonitoring Intra Operatif: Mindi Widayani NRP 122.022.1115 FK UPN "Veteran" Jakartaputri wulandariPas encore d'évaluation
- Hukum CourvoisierDocument1 pageHukum CourvoisierFahryHamkaPas encore d'évaluation
- Spesifikasi - Fukuda FX-8400Document1 pageSpesifikasi - Fukuda FX-8400Dony Aji SPas encore d'évaluation
- COMFORT ScaleDocument7 pagesCOMFORT ScaleALDO STEFANUZ (STIK)Pas encore d'évaluation
- Pendant Series One MedDocument10 pagesPendant Series One MedHesti HerawatiPas encore d'évaluation
- Ventilator Alarms and TroubleshootingDocument23 pagesVentilator Alarms and Troubleshootingjanubiomed0209100% (1)
- Ventilator Draeger Evita V300 - Spesifikasi Teknis PDFDocument4 pagesVentilator Draeger Evita V300 - Spesifikasi Teknis PDFArifyadin SudonoPas encore d'évaluation
- Perhitungan Beban Kerja IPS MedisDocument55 pagesPerhitungan Beban Kerja IPS Medisainul istiadzahPas encore d'évaluation
- THT Bimbel Ukdi Mantap 2015 - NorestrictionDocument227 pagesTHT Bimbel Ukdi Mantap 2015 - NorestrictionpanduPas encore d'évaluation
- Kuliah Extrapyramidal SyndromeDocument50 pagesKuliah Extrapyramidal SyndromePutri Azka RinandaPas encore d'évaluation
- JPP Self HarmDocument10 pagesJPP Self Harmluthfi anggia sastiwi0% (1)
- Pengaruh Pemberian Infus Hangat Terhadap Stabilitas Suhu Tubuh Pada Pasien Post Operasi General Anestesi Di Recovery Room Rsu Karsa Husada BatuDocument7 pagesPengaruh Pemberian Infus Hangat Terhadap Stabilitas Suhu Tubuh Pada Pasien Post Operasi General Anestesi Di Recovery Room Rsu Karsa Husada BatuKonsul Dosen PembibingPas encore d'évaluation
- GelafusalinfDocument5 pagesGelafusalinfToni Dafia PutraPas encore d'évaluation
- Pain Assessment Worksheet IntermediateDocument5 pagesPain Assessment Worksheet Intermediatekelly_aslanidouPas encore d'évaluation
- Emailing Patologi Anatomi GANGGUAN HEMODINAMIK Trombosis DAN SHOCK - Output PDFDocument38 pagesEmailing Patologi Anatomi GANGGUAN HEMODINAMIK Trombosis DAN SHOCK - Output PDFHaykal FathirrahmanPas encore d'évaluation
- Defibrilator PDFDocument30 pagesDefibrilator PDFSkolastika gangguPas encore d'évaluation
- IPSG ChapterDocument52 pagesIPSG Chaptersyahrul muhammadPas encore d'évaluation
- Alat Untuk Mengukur Kedalaman AnestesiDocument3 pagesAlat Untuk Mengukur Kedalaman AnestesiditaPas encore d'évaluation
- Pemeriksaan Refleks BulbocavernosusDocument2 pagesPemeriksaan Refleks BulbocavernosusAnonymous h0DxuJTPas encore d'évaluation
- Tehnik - Tehnik Analgesia Post OperasiDocument32 pagesTehnik - Tehnik Analgesia Post OperasiGuntur Aryo PuntodewoPas encore d'évaluation
- Extubation Criteria & Delayed EmergenceDocument3 pagesExtubation Criteria & Delayed EmergenceAnonymous OlS0WZwPas encore d'évaluation
- Jumlah Tetesan Infus MakroDocument2 pagesJumlah Tetesan Infus MakroMamanya Ef Taya ThalitaPas encore d'évaluation
- Guideline - Training New Trainer ISMKI 2016Document18 pagesGuideline - Training New Trainer ISMKI 2016Dhery Dev WhitterPas encore d'évaluation
- Analgesi Dan Sedasi Di IcuDocument32 pagesAnalgesi Dan Sedasi Di IcuWidi Yuli HariantoPas encore d'évaluation
- Tabel Konversi FiO2Document2 pagesTabel Konversi FiO2arie_yuliantoPas encore d'évaluation
- 2018 Farmakoterapi Obat-Obatan Emergency v2Document90 pages2018 Farmakoterapi Obat-Obatan Emergency v2saifudinPas encore d'évaluation
- AnestesiDocument11 pagesAnestesiAnonymous 8w9QEGPas encore d'évaluation
- Vascular Acces in Hemodyalisi - DR DjoniDocument50 pagesVascular Acces in Hemodyalisi - DR DjoniMohamad ZulfikarPas encore d'évaluation
- CombinedDocument3 pagesCombinedSolape Akin-WilliamsPas encore d'évaluation
- General Anesthesia 2021Document89 pagesGeneral Anesthesia 2021helda dwianaPas encore d'évaluation
- DruggggggDocument43 pagesDruggggggmonesabiancaPas encore d'évaluation
- Assignment AnesthesiaDocument9 pagesAssignment AnesthesiaRavi PatelPas encore d'évaluation
- PharmacologyDocument27 pagesPharmacologyKyla CastroPas encore d'évaluation
- AnesthesiaDocument49 pagesAnesthesiaboboPas encore d'évaluation
- Anesthetics BothDocument36 pagesAnesthetics BothDeribe BekelePas encore d'évaluation
- 7 PhysioloDocument51 pages7 PhysioloNia HndynPas encore d'évaluation
- Making Oral Presentation-3Document39 pagesMaking Oral Presentation-3Nia HndynPas encore d'évaluation
- Hemodynamic MonitoringDocument89 pagesHemodynamic MonitoringNia HndynPas encore d'évaluation
- Sindroma Koroner AkutDocument28 pagesSindroma Koroner AkutNia HndynPas encore d'évaluation
- Simulation of A Snake RobotDocument61 pagesSimulation of A Snake Robotmuhammed inzamamPas encore d'évaluation
- Grimshaw v. Ford Motor CoDocument35 pagesGrimshaw v. Ford Motor CozichenPas encore d'évaluation
- Appraisal: Gilmore and Williams: Human Resource ManagementDocument18 pagesAppraisal: Gilmore and Williams: Human Resource ManagementShilpa GorePas encore d'évaluation
- MEM Companion Volume Implementation Guide - Release 1.1Document23 pagesMEM Companion Volume Implementation Guide - Release 1.1Stanley AlexPas encore d'évaluation
- Fujiwheel CatalogDocument16 pagesFujiwheel CatalogKhaeri El BarbasyPas encore d'évaluation
- A Plan of Life - Scepter BookletDocument10 pagesA Plan of Life - Scepter Bookletpeteatkinson@gmail.comPas encore d'évaluation
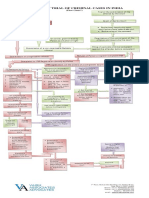
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 pageProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- 13 Reasons Why Discussion GuideDocument115 pages13 Reasons Why Discussion GuideEC Pisano RiggioPas encore d'évaluation
- 39 Storey Treehouse Activity Pack PDFDocument11 pages39 Storey Treehouse Activity Pack PDFNeptune Shell0% (3)
- Time Value of Money PDFDocument4 pagesTime Value of Money PDFCalvin SandiPas encore d'évaluation
- Untitled PresentationDocument23 pagesUntitled Presentationapi-543394268Pas encore d'évaluation
- The Value Relevance of Financial Statements and Their Impact On Stock PricesDocument18 pagesThe Value Relevance of Financial Statements and Their Impact On Stock Pricesanubha srivastavaPas encore d'évaluation
- Unit Test 9 BDocument1 pageUnit Test 9 BAnnaPas encore d'évaluation
- List - of - Members As On 6 3 18 PDFDocument8 pagesList - of - Members As On 6 3 18 PDFashish jaiswal100% (1)
- Sec A - Group 9 - When A New Manager StumblesDocument13 pagesSec A - Group 9 - When A New Manager StumblesVijay Krishnan100% (3)
- 659.69 BM67 2018-02-06 02 Im Beu-UsaDocument88 pages659.69 BM67 2018-02-06 02 Im Beu-UsaIrakli JibladzePas encore d'évaluation
- A Comparative Study of Intelligence in Children of Consanguineous and Non-Consanguineous Marriages and Its Relationship With Holland's Personality Types in High School Students of TehranDocument8 pagesA Comparative Study of Intelligence in Children of Consanguineous and Non-Consanguineous Marriages and Its Relationship With Holland's Personality Types in High School Students of TehranInternational Medical PublisherPas encore d'évaluation
- Atf Fire Research Laboratory - Technical Bulletin 02 0Document7 pagesAtf Fire Research Laboratory - Technical Bulletin 02 0Mauricio Gallego GilPas encore d'évaluation
- Form Seven PlacementsDocument26 pagesForm Seven PlacementsRL Iroga100% (4)
- Rice and Contract TermsDocument7 pagesRice and Contract TermsMilling and Grain magazinePas encore d'évaluation
- Flex Li3 21 VAADocument1 pageFlex Li3 21 VAAAyman Al-YafeaiPas encore d'évaluation
- Akshaya Tritya! One of The Ancient Festivals of IndiaDocument9 pagesAkshaya Tritya! One of The Ancient Festivals of IndiaHoracio TackanooPas encore d'évaluation
- Infor LN Baan - Debugging The BshellDocument26 pagesInfor LN Baan - Debugging The BshellShiva KumarPas encore d'évaluation
- Math9 - Q2 - Mod2 - WK 3 - JointAndCombinedVariations - Version2Document37 pagesMath9 - Q2 - Mod2 - WK 3 - JointAndCombinedVariations - Version2Precious Arni100% (7)
- Kenya's Top 10 Tourist SpotsDocument23 pagesKenya's Top 10 Tourist SpotsAaron LopezPas encore d'évaluation
- El Poder de La Disciplina El Hábito Que Cambiará Tu Vida (Raimon Samsó)Document4 pagesEl Poder de La Disciplina El Hábito Que Cambiará Tu Vida (Raimon Samsó)ER CaballeroPas encore d'évaluation
- Commercial Dispatch Eedition 6-13-19Document12 pagesCommercial Dispatch Eedition 6-13-19The Dispatch100% (1)
- 2020 DepEd English Proficiency Test (EPT) Reviewer - TeacherPHDocument205 pages2020 DepEd English Proficiency Test (EPT) Reviewer - TeacherPHAlron GAmboa100% (1)
- Igice Cya Kabiri: 2.0. Intambwe Zitandukanye Z'Imikorere Ya Mariyamu KinyamaruraDocument7 pagesIgice Cya Kabiri: 2.0. Intambwe Zitandukanye Z'Imikorere Ya Mariyamu KinyamaruraJacques Abimanikunda BarahirwaPas encore d'évaluation
- Microwave Oven: Instructions & Cooking GuideDocument38 pagesMicrowave Oven: Instructions & Cooking GuidethomaselandPas encore d'évaluation