Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Maternal Injuries During Vaginal Delivery and Its ManagementDocument51 pagesMaternal Injuries During Vaginal Delivery and Its ManagementJay Seetohul100% (1)
- Perineal Care ModuleDocument7 pagesPerineal Care ModuleHEIDE BASING-APas encore d'évaluation
- Procedures in Obstetrics and Gynaecology TextbookDocument272 pagesProcedures in Obstetrics and Gynaecology TextbookPriyaPas encore d'évaluation
- Ian M Symonds Sabaratnam Arulkumaran E M Symonds Essential Obstetrics and GynaecologyDocument449 pagesIan M Symonds Sabaratnam Arulkumaran E M Symonds Essential Obstetrics and GynaecologyOrlando Butnariu100% (2)
- Lecture-33 Postpartum HemorrhageDocument50 pagesLecture-33 Postpartum HemorrhageMadhu Sudhan Pandeya100% (2)
- Perineal Massage in PregnancyDocument2 pagesPerineal Massage in PregnancyAbanbesarPas encore d'évaluation
- Lecture-35 Eectronic Fetal MonitoringDocument45 pagesLecture-35 Eectronic Fetal MonitoringMadhu Sudhan PandeyaPas encore d'évaluation
- Perineal CareDocument19 pagesPerineal CareGracy Morada Cu100% (3)
- Lecture-28 Placenta PreviaDocument43 pagesLecture-28 Placenta PreviaMadhu Sudhan Pandeya100% (1)
- Nursing Care PlanDocument7 pagesNursing Care PlanDickson,Emilia Jade100% (3)
- Fetal DistressDocument32 pagesFetal DistressMadhu Sudhan PandeyaPas encore d'évaluation
- Ob - Abnormalities of The Third Stage of Labor andDocument108 pagesOb - Abnormalities of The Third Stage of Labor andapi-3856051100% (2)
- Traumatic PPHDocument30 pagesTraumatic PPHRizwana BanuPas encore d'évaluation
- Abortion: Renhe Hospital Wang JunjieDocument51 pagesAbortion: Renhe Hospital Wang JunjieMadhu Sudhan PandeyaPas encore d'évaluation
- Quick Guide For Candidates: Step 1: Creating An Account and Logging in Create An AccountDocument2 pagesQuick Guide For Candidates: Step 1: Creating An Account and Logging in Create An AccountMadhu Sudhan Pandeya100% (1)
- Voter ListDocument214 pagesVoter ListMadhu Sudhan PandeyaPas encore d'évaluation
- श्रम एेन २०७४Document53 pagesश्रम एेन २०७४PradIpta Kaphle0% (1)
- Nepal Medical Council Act, 2020 (1964)Document20 pagesNepal Medical Council Act, 2020 (1964)Madhu Sudhan PandeyaPas encore d'évaluation
- Who Rights Roles Respon HW Covid 19Document3 pagesWho Rights Roles Respon HW Covid 19HarryPas encore d'évaluation
- Teratology & Chronic PoisoningDocument54 pagesTeratology & Chronic PoisoningMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture-11 Breech PresentationDocument27 pagesLecture-11 Breech PresentationMadhu Sudhan PandeyaPas encore d'évaluation
- Vaccination Guideline: International Travel and Health 2007Document9 pagesVaccination Guideline: International Travel and Health 2007Madhu Sudhan PandeyaPas encore d'évaluation
- Lecture-18 Obstructed LaborDocument8 pagesLecture-18 Obstructed LaborMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture-31 Instrumental DeliveryDocument33 pagesLecture-31 Instrumental DeliveryMadhu Sudhan PandeyaPas encore d'évaluation
- Bishop's Pre-Induction Cervical Scoring SystemDocument2 pagesBishop's Pre-Induction Cervical Scoring SystemMadhu Sudhan PandeyaPas encore d'évaluation
- Postpartum Hemorrhage: The First Clinical College of Three Gorges University, Wang XiaojinDocument98 pagesPostpartum Hemorrhage: The First Clinical College of Three Gorges University, Wang XiaojinMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture-22 Prolonged PregnancyDocument24 pagesLecture-22 Prolonged PregnancyMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture 30 PromDocument7 pagesLecture 30 PromMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture-25 Cesarean SectionDocument21 pagesLecture-25 Cesarean SectionMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture-26 Hypertensive Disease of PregnancyDocument28 pagesLecture-26 Hypertensive Disease of PregnancyMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture-13 Transeverse LieDocument15 pagesLecture-13 Transeverse LieMadhu Sudhan PandeyaPas encore d'évaluation
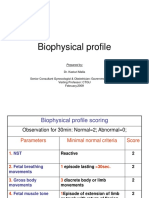
- Lecture-23 Biophysical ProfieDocument3 pagesLecture-23 Biophysical ProfieMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture-17 Shoulder DystociaDocument20 pagesLecture-17 Shoulder DystociaMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture-27 Ectopic PregnancyDocument38 pagesLecture-27 Ectopic PregnancyMadhu Sudhan PandeyaPas encore d'évaluation
- Cord ProlapseDocument7 pagesCord ProlapseMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture-12 Face PresentationDocument9 pagesLecture-12 Face PresentationMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture-6 Obstetric TerminologiesDocument17 pagesLecture-6 Obstetric TerminologiesMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture-15 Prolonged LaborDocument8 pagesLecture-15 Prolonged LaborMadhu Sudhan PandeyaPas encore d'évaluation
- Lecture-24 Twins PregnancyDocument30 pagesLecture-24 Twins PregnancyMadhu Sudhan PandeyaPas encore d'évaluation
- GynecoDocument3 pagesGynecoanne laurePas encore d'évaluation
- Sutingco ESSAY PERICAREDocument2 pagesSutingco ESSAY PERICAREMary SutingcoPas encore d'évaluation
- OBGYN Practice - Bulletin - No - 165 - Prevention - And.46Document15 pagesOBGYN Practice - Bulletin - No - 165 - Prevention - And.46Mia FernandezPas encore d'évaluation
- Byung Kang Pelvis 09.15.2014Document121 pagesByung Kang Pelvis 09.15.2014Elena ConstantinPas encore d'évaluation
- Genital Prolapse: Unit - V 2K15Document58 pagesGenital Prolapse: Unit - V 2K15sushma nakkinaPas encore d'évaluation
- Single-Knot Versus Multiple-Knot Technique of Perineal Repair - A Randomised Controlled TrialDocument8 pagesSingle-Knot Versus Multiple-Knot Technique of Perineal Repair - A Randomised Controlled TrialDR RISKA WAHYUPas encore d'évaluation
- كتاب اسئلة جميلDocument401 pagesكتاب اسئلة جميلMohammadSAL-Rawashdeh100% (1)
- How To Repair An Episiotomy: Clinical SkillsDocument4 pagesHow To Repair An Episiotomy: Clinical SkillsLuna JessicaPas encore d'évaluation
- Perineal CareDocument2 pagesPerineal CareneehoshiPas encore d'évaluation
- Question No 01: PART A) Define Pelvis?Document5 pagesQuestion No 01: PART A) Define Pelvis?aminaPas encore d'évaluation
- OgenisisDocument52 pagesOgenisisBharat ThapaPas encore d'évaluation
- Textbook of Obstetrics & GynecologyDocument37 pagesTextbook of Obstetrics & Gynecologysanjivdas0% (1)
- PERILITE and HOT SITZDocument3 pagesPERILITE and HOT SITZMikha BorcesPas encore d'évaluation
- Normal Labour 400lDocument102 pagesNormal Labour 400lAbdullahi Suleiman MakaPas encore d'évaluation
- MCN Reviewer DefinitionOfTermsDocument10 pagesMCN Reviewer DefinitionOfTermsJenessel Ann P DaugPas encore d'évaluation
- Jigjiga University: Anatomy of PerineumDocument114 pagesJigjiga University: Anatomy of PerineumKamal AhmedPas encore d'évaluation
- Birth Canal Injuries Final LectureDocument28 pagesBirth Canal Injuries Final LectureAnjali Rahul AjmeriPas encore d'évaluation
- NCM 107 SKL FinalsDocument33 pagesNCM 107 SKL FinalsCyriz Ann Mae PacisPas encore d'évaluation
- BACA Programme July 08Document30 pagesBACA Programme July 08ready medicPas encore d'évaluation
- Dyspareunia Following Childbirth: Christine Kettle, Khaled Ismail and Fidelma O'MahonyDocument5 pagesDyspareunia Following Childbirth: Christine Kettle, Khaled Ismail and Fidelma O'MahonygedePas encore d'évaluation
- MCQS, PelvisDocument23 pagesMCQS, PelvisICIKITI JOELPas encore d'évaluation