Vous aimerez peut-être aussi
- Assessment of PainDocument4 pagesAssessment of PaingwapdosePas encore d'évaluation
- The COAT & Review Approach: How to recognise and manage unwell patientsD'EverandThe COAT & Review Approach: How to recognise and manage unwell patientsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Continuous Renal Replacement Therapy (CRRT) Initial Competency Assessment and ValidationDocument2 pagesContinuous Renal Replacement Therapy (CRRT) Initial Competency Assessment and Validationalex100% (1)
- 3 Sentinel Event Reporting Form (SERF) .Document2 pages3 Sentinel Event Reporting Form (SERF) .aameeenPas encore d'évaluation
- Audit assessing aspirin use in angina patientsDocument3 pagesAudit assessing aspirin use in angina patientsbalaji srinivasanPas encore d'évaluation
- Quality Indicators For ICU: Indian Society of Critical Care Medicine 2009Document61 pagesQuality Indicators For ICU: Indian Society of Critical Care Medicine 2009akinravPas encore d'évaluation
- s6 Clinical HandoverDocument26 pagess6 Clinical HandoverirenediahjPas encore d'évaluation
- Departmental Nursing Orientation ChecklistDocument2 pagesDepartmental Nursing Orientation ChecklistMero Hassan50% (2)
- Emergency Admission & Transfer Register RecordsDocument21 pagesEmergency Admission & Transfer Register RecordsAnkur Singh0% (1)
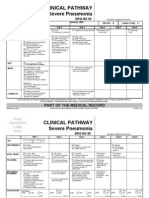
- Clinical Pathways Severe PneumoniaDocument2 pagesClinical Pathways Severe PneumoniaaandakuPas encore d'évaluation
- Emergency Department PolicyDocument18 pagesEmergency Department PolicySt. Mary's HospitalPas encore d'évaluation
- Pediatric Early Warning ScorecardDocument1 pagePediatric Early Warning ScorecardMuh NatsirPas encore d'évaluation
- Code Blue Form DocumentationDocument2 pagesCode Blue Form DocumentationRaviraj Pishe89% (9)
- Registration FormDocument5 pagesRegistration FormSreejith Kelakam100% (1)
- NABH Accreditation Criteria OverviewDocument8 pagesNABH Accreditation Criteria Overviewdhir.ankurPas encore d'évaluation
- Tata Motors Hospital ICU Quality AssuranceDocument10 pagesTata Motors Hospital ICU Quality AssuranceAniruddha ChatterjeePas encore d'évaluation
- DH Ratnagiri Quality ManualDocument71 pagesDH Ratnagiri Quality ManualPrabhat Kumar100% (2)
- Kayakalp Standards NABHDocument18 pagesKayakalp Standards NABHSwati BajpaiPas encore d'évaluation
- OP 4070 Reporting of OVADocument17 pagesOP 4070 Reporting of OVAAhmed HannoPas encore d'évaluation
- Nursing ICUDocument2 pagesNursing ICUKomal Tomar50% (2)
- 5 Labour Room Laqshya Assessment ToolkitDocument16 pages5 Labour Room Laqshya Assessment ToolkitAnjali Rahul Ajmeri50% (2)
- Nabh IdicatorsDocument61 pagesNabh IdicatorsStacy King100% (5)
- Quality Indicators 5th Edition WordDocument14 pagesQuality Indicators 5th Edition WordtanishaPas encore d'évaluation
- NPS - Patient Feedback FormDocument1 pageNPS - Patient Feedback FormNatasha BhasinPas encore d'évaluation
- APP-KSMC-127 - (V4) - Crash Cart Checking & Maintenance Rev120314Document8 pagesAPP-KSMC-127 - (V4) - Crash Cart Checking & Maintenance Rev120314Kimberly Solis100% (2)
- Additional Questions AnsweredDocument5 pagesAdditional Questions AnsweredS D50% (2)
- ICN Nurse Job ResponsibilitiesDocument2 pagesICN Nurse Job ResponsibilitiesBirupakshya RoutPas encore d'évaluation
- Privileging - Resident Medical OfficerDocument6 pagesPrivileging - Resident Medical OfficerAjaiwant CheemaPas encore d'évaluation
- Patient Health ProfileDocument4 pagesPatient Health ProfileChristopher WuPas encore d'évaluation
- CQE 7 Nursing Quality Indicators 1Document24 pagesCQE 7 Nursing Quality Indicators 1Inder Singh YadavPas encore d'évaluation
- Patient Handover AuditDocument2 pagesPatient Handover AuditTni Jolie75% (4)
- IPSGDocument4 pagesIPSGmohsinaPas encore d'évaluation
- Manage code blue patient documentationDocument1 pageManage code blue patient documentationHendra KurniawanPas encore d'évaluation
- Cbahi Jan 19 Ovr Risk SafetyDocument52 pagesCbahi Jan 19 Ovr Risk SafetyMunaPas encore d'évaluation
- INDICATORSDocument15 pagesINDICATORSMonish ParmarPas encore d'évaluation
- 93 - Operating Room ProtocolDocument25 pages93 - Operating Room ProtocolFelix Kwenandar100% (1)
- Patient Identification PolicyDocument20 pagesPatient Identification PolicyZahwa DhiyanaPas encore d'évaluation
- Integrated Cath Lab Safety ChecklistDocument2 pagesIntegrated Cath Lab Safety ChecklistwenhalPas encore d'évaluation
- SHCO Standards - 3rd EditionDocument188 pagesSHCO Standards - 3rd Editionrenu100% (2)
- Guide To Clinical Audit Antibiotic Use in Urinary Tract InfectionDocument10 pagesGuide To Clinical Audit Antibiotic Use in Urinary Tract Infectionihtisham1Pas encore d'évaluation
- Management of MedicationDocument32 pagesManagement of Medicationsanjay100% (1)
- Scope of ServiceDocument7 pagesScope of ServiceSN Malenadu CreationPas encore d'évaluation
- PROJECT CHARTER Pressure UlcerDocument2 pagesPROJECT CHARTER Pressure UlcerQuality PmnhPas encore d'évaluation
- New Objective Elements 5th Edition of NABHDocument7 pagesNew Objective Elements 5th Edition of NABHsoni100% (1)
- Maintenance of Patients Records, Its Security, Sharing of Information and Safe DisposalDocument7 pagesMaintenance of Patients Records, Its Security, Sharing of Information and Safe DisposalAjay KumarPas encore d'évaluation
- CBAHI Standard Chapter 2 Medical Staff Provision CareDocument14 pagesCBAHI Standard Chapter 2 Medical Staff Provision CareAhmed Attia100% (2)
- 0 - 16 03 24 Provincial PEWS Nursing Power Point MarchDocument30 pages0 - 16 03 24 Provincial PEWS Nursing Power Point MarchfannyPas encore d'évaluation
- Essential Safety Requirements - (Esr) Standards For Saudi Cbahi Accreditation in Hospitals and Phc'S. Gdharr Riyadh Saudi ArabiaDocument36 pagesEssential Safety Requirements - (Esr) Standards For Saudi Cbahi Accreditation in Hospitals and Phc'S. Gdharr Riyadh Saudi Arabiarelena badr100% (1)
- Nabh FormDocument14 pagesNabh Formakshay ranePas encore d'évaluation
- JCI 2017 IPSG Infographic 062017 PDFDocument1 pageJCI 2017 IPSG Infographic 062017 PDFknotstmPas encore d'évaluation
- Initial Assessment Form Specialist OPDDocument1 pageInitial Assessment Form Specialist OPDvicndub100% (1)
- HIRA For Patient Safety Check Risk - FinalDocument10 pagesHIRA For Patient Safety Check Risk - FinalMelvin DsouzaPas encore d'évaluation
- Post Anesthesia Care Unit RecordDocument1 pagePost Anesthesia Care Unit RecordDamien Marwein100% (1)
- Gap Analysis Report For Health Care Organnization (Hco) Hospital ProfileDocument7 pagesGap Analysis Report For Health Care Organnization (Hco) Hospital ProfileDhananjay SainiPas encore d'évaluation
- Mortuary Services Checklist - Random 202335531Document4 pagesMortuary Services Checklist - Random 202335531Marion KonesPas encore d'évaluation
- PfeDocument2 pagesPfeCaryl Lou Casamayor100% (3)
- IcuDocument8 pagesIcuBikul Nayar100% (1)
- Management of Tuberculosis: A guide for clinicians (eBook edition)D'EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Pas encore d'évaluation
- INFECTION CONTROL: Passbooks Study GuideD'EverandINFECTION CONTROL: Passbooks Study GuidePas encore d'évaluation
- Cancer Pain ManagementDocument48 pagesCancer Pain ManagementRifka Septia PutriPas encore d'évaluation
- Legalization of MarijuanaDocument18 pagesLegalization of MarijuanaCarlo Troy AcelottPas encore d'évaluation
- Chronic Kidney DiseaseDocument37 pagesChronic Kidney DiseaseHikmah Ilyas El-LuthanyPas encore d'évaluation
- Igas Flow ChartDocument1 pageIgas Flow ChartYi Wei KoPas encore d'évaluation
- Anemia of Prematurity UpToDate PDFDocument13 pagesAnemia of Prematurity UpToDate PDFАлександар ТасићPas encore d'évaluation
- Recommendation Letter - SheriDocument1 pageRecommendation Letter - Sheriapi-355180754100% (1)
- Medical-Surgical Questions With Rationale 70 QuestionsDocument59 pagesMedical-Surgical Questions With Rationale 70 QuestionsJam Torres100% (7)
- APA - DSM 5 Depression Bereavement Exclusion PDFDocument2 pagesAPA - DSM 5 Depression Bereavement Exclusion PDFDaniel NgPas encore d'évaluation
- Optical Correction of Aphakia in Children: Review ArticleDocument12 pagesOptical Correction of Aphakia in Children: Review Articleaisa mutiaraPas encore d'évaluation
- Socolov Et. Al., 2018 Cognitive Impairment in MEDocument19 pagesSocolov Et. Al., 2018 Cognitive Impairment in MERicardo Jose De LeonPas encore d'évaluation
- Child and AdolescentDocument86 pagesChild and AdolescentMichelle RamosPas encore d'évaluation
- Elizabeth Resume 2Document3 pagesElizabeth Resume 2api-252417118Pas encore d'évaluation
- Using Lean Six Sigma Techniques To Improve Efficiency in Outpatient Ophthalmology ClinicsDocument9 pagesUsing Lean Six Sigma Techniques To Improve Efficiency in Outpatient Ophthalmology ClinicsMinh Nguyễn Phương HồngPas encore d'évaluation
- What Do Language Disorders Reveal About Brain-Language Relationships? From Classic Models To Network ApproachesDocument14 pagesWhat Do Language Disorders Reveal About Brain-Language Relationships? From Classic Models To Network ApproachesvalentinepoulainPas encore d'évaluation
- Perloff TOFDocument28 pagesPerloff TOFvamshidhPas encore d'évaluation
- SCHEDULE OPTIMIZEDDocument2 pagesSCHEDULE OPTIMIZEDAnonymous iScW9lPas encore d'évaluation
- CPR GuidelinesDocument30 pagesCPR GuidelineswvhvetPas encore d'évaluation
- 2013 Fluconazole Resistant Candida Albicans.22Document8 pages2013 Fluconazole Resistant Candida Albicans.22Kala SuvarnaPas encore d'évaluation
- HCW NigeriaDocument12 pagesHCW NigeriaFrancis Njihia KaburuPas encore d'évaluation
- Anaesthetic Drug Crib Sheet-8 PDFDocument1 pageAnaesthetic Drug Crib Sheet-8 PDFLiam O'ConnorPas encore d'évaluation
- Mnemonic Devices for Medical EducationDocument9 pagesMnemonic Devices for Medical EducationJhey MalanyaonPas encore d'évaluation
- GNMK IMC 20152 A EPlex BrochureDocument4 pagesGNMK IMC 20152 A EPlex BrochureBilgi KurumsalPas encore d'évaluation
- APLS Scenario OSCE PDFDocument5 pagesAPLS Scenario OSCE PDFNikita JacobsPas encore d'évaluation
- Katzung SummaryDocument60 pagesKatzung Summaryedwarbc1Pas encore d'évaluation
- SURGERY Lecture 2 - Liver & Gallbladder (Dr. Wenceslao)Document19 pagesSURGERY Lecture 2 - Liver & Gallbladder (Dr. Wenceslao)Medisina101100% (1)
- A Placebo-Controlled Test of Cognitive-Behavioral Therapy For Comorbid Insomnia in Older AdultsDocument11 pagesA Placebo-Controlled Test of Cognitive-Behavioral Therapy For Comorbid Insomnia in Older Adultssilvia dwi puspitaPas encore d'évaluation
- UG Curriculum Vol II PDFDocument247 pagesUG Curriculum Vol II PDFRavi Meher67% (3)
- Depression DOHDocument4 pagesDepression DOHnut_crackrePas encore d'évaluation
- NCP: Labor Stage 1 Latent PhaseDocument9 pagesNCP: Labor Stage 1 Latent PhaseJaviePas encore d'évaluation
- Patient care and discharge planDocument2 pagesPatient care and discharge planBryan Carmona100% (1)
- Facial Trauma - Seth Thaller, W. Scott McDonaldDocument491 pagesFacial Trauma - Seth Thaller, W. Scott McDonaldMirela Nazaru-Manole50% (2)