Vous aimerez peut-être aussi
- Physical Examination of The Knee: Oleh: Dr. Feby Deliana Pembimbing: Dr. Deta Tanuwidjadja.,SpkfrDocument25 pagesPhysical Examination of The Knee: Oleh: Dr. Feby Deliana Pembimbing: Dr. Deta Tanuwidjadja.,Spkfrsingle_ladyPas encore d'évaluation
- Special Test KNEE UnaDocument25 pagesSpecial Test KNEE Unasingle_ladyPas encore d'évaluation
- Knee (Word)Document18 pagesKnee (Word)dwPas encore d'évaluation
- Orthopaedic Special TestDocument24 pagesOrthopaedic Special TestpradhanaadhityaPas encore d'évaluation
- Ankleand FootDocument35 pagesAnkleand FootHeba Abo bakrPas encore d'évaluation
- Assessment MusculoskeletalDocument6 pagesAssessment Musculoskeletaldd marshall100% (1)
- Spine Exam 2Document44 pagesSpine Exam 2Azmi FarhadiPas encore d'évaluation
- HerniaDocument62 pagesHerniaBen IntosiusPas encore d'évaluation
- Upper & Lower Limb ExaminationDocument20 pagesUpper & Lower Limb Examinationcvmqx7yppd100% (1)
- Foot and Ankle BiomechanicsDocument25 pagesFoot and Ankle BiomechanicsSanh NguyễnPas encore d'évaluation
- 5 - Knee DisordersDocument85 pages5 - Knee Disordersraed faisalPas encore d'évaluation
- The HipsDocument2 pagesThe HipsReham QuePas encore d'évaluation
- Examination of The KneeDocument5 pagesExamination of The KneenushPas encore d'évaluation
- AnD FT Elbow-1Document26 pagesAnD FT Elbow-1Nazwa KamilatunnisaPas encore d'évaluation
- Ankylosing Spondylitis 1Document31 pagesAnkylosing Spondylitis 1Salman KhanPas encore d'évaluation
- Assessment of MS SystemDocument68 pagesAssessment of MS Systemdileepkumar.duhs4817Pas encore d'évaluation
- Elbow AssessmentDocument39 pagesElbow AssessmentshizarahimPas encore d'évaluation
- Pemeriksaan Fisik LututDocument54 pagesPemeriksaan Fisik LututShone NamPas encore d'évaluation
- Reflex TestingDocument44 pagesReflex Testingsarguss14100% (7)
- Ulnar Nerve Entrapment at The ElbowDocument19 pagesUlnar Nerve Entrapment at The ElbowChristian SolihinPas encore d'évaluation
- KneeDocument29 pagesKneedoctoradeeb18Pas encore d'évaluation
- Musculoskeletal Examination Under GraduatesDocument98 pagesMusculoskeletal Examination Under GraduatesEsraa SalemPas encore d'évaluation
- Assessment of The Musculo-Skeletal SystemDocument46 pagesAssessment of The Musculo-Skeletal SystemRaquel M. MendozaPas encore d'évaluation
- Knee, Ankle and Foot Joint MobilizationDocument17 pagesKnee, Ankle and Foot Joint MobilizationLokesh SharmaPas encore d'évaluation
- MSK Physical Examination - Part 2Document82 pagesMSK Physical Examination - Part 2loveakaylaquinnPas encore d'évaluation
- Clinical Examinations For PLAB 2Document12 pagesClinical Examinations For PLAB 2Mandeep KaurPas encore d'évaluation
- Musculoskeletal System Health Assessment LectureDocument66 pagesMusculoskeletal System Health Assessment LectureMikylla OrdanielPas encore d'évaluation
- Kinesiologi Siku-Pf UnaDocument59 pagesKinesiologi Siku-Pf Unasingle_ladyPas encore d'évaluation
- Omm Exam 3 LGTDocument59 pagesOmm Exam 3 LGTSolomon Seth SallforsPas encore d'évaluation
- Hip, Knee, Ankle PROMDocument28 pagesHip, Knee, Ankle PROMsxsparsh2305Pas encore d'évaluation
- Musculoskeletal System Name-Purushothaman Sabarigiri 1 Year Sec - IDocument31 pagesMusculoskeletal System Name-Purushothaman Sabarigiri 1 Year Sec - INuhu BankwhotPas encore d'évaluation
- Physical Examination GI Track (INTERNATIONAL)Document59 pagesPhysical Examination GI Track (INTERNATIONAL)AnnisPas encore d'évaluation
- Musculoskeletal SystemDocument160 pagesMusculoskeletal SystemAirene Aquino BusaniaPas encore d'évaluation
- Hip and Buttock PainDocument26 pagesHip and Buttock PainEdy SetiawanPas encore d'évaluation
- Hernia & PR: DR - Abdulwahid M Salih M.D. SurgeryDocument38 pagesHernia & PR: DR - Abdulwahid M Salih M.D. SurgeryumiumiPas encore d'évaluation
- 10 +Manual+Muscle+Testing+of+the+Ankle+Plantar+FlexionDocument36 pages10 +Manual+Muscle+Testing+of+the+Ankle+Plantar+FlexionzelinaokiPas encore d'évaluation
- An Orthopedic Treatment That Involves Placing On A Limb, Bone or Muscle Group Using Variety ofDocument22 pagesAn Orthopedic Treatment That Involves Placing On A Limb, Bone or Muscle Group Using Variety oflemuel_que100% (2)
- Assessing The NeckDocument3 pagesAssessing The NeckAnne Joyce Lara AlbiosPas encore d'évaluation
- Assessment of Nutritional Status and Presence of MalnutritionDocument13 pagesAssessment of Nutritional Status and Presence of MalnutritionFT YPas encore d'évaluation
- Nerve Courses and PalpationsDocument11 pagesNerve Courses and PalpationsSarin AvniPas encore d'évaluation
- 5-Flexibility TestsDocument62 pages5-Flexibility TestsMr. MixerPas encore d'évaluation
- YEAR 1 and 2 OSCE Revision: Author: DR Thomas PayneDocument30 pagesYEAR 1 and 2 OSCE Revision: Author: DR Thomas Payneminayoki100% (1)
- MuscleDocument38 pagesMuscleAnonymous BzS0RF1qyPas encore d'évaluation
- Spondylolysis SpondylolisthesisDocument89 pagesSpondylolysis SpondylolisthesisAh ZhangPas encore d'évaluation
- Malunion and Non-UnionDocument12 pagesMalunion and Non-UnionHengkai NeoPas encore d'évaluation
- Approach To ArthralgiaDocument5 pagesApproach To ArthralgiaBlaire FultonePas encore d'évaluation
- Respiratory Examination GuideDocument4 pagesRespiratory Examination Guiderhea100% (2)
- 4-Anatomy of The ForearmDocument31 pages4-Anatomy of The ForearmMuostafa KamelPas encore d'évaluation
- CH 3 - PT 2Document22 pagesCH 3 - PT 2noureenPas encore d'évaluation
- Anatomy of The SpineDocument61 pagesAnatomy of The SpineAnonymous 9XDi2Yqa0% (2)
- 7 Muscle Length TestingDocument8 pages7 Muscle Length Testingbuhlembatha304Pas encore d'évaluation
- Elbow PT AssessmentDocument31 pagesElbow PT Assessmentkrissh20Pas encore d'évaluation
- CMR of Hip Dislocation and Shoulder RomeoDocument21 pagesCMR of Hip Dislocation and Shoulder RomeoHarith ShahiranPas encore d'évaluation
- 9 HerniaDocument38 pages9 HerniaErwin SiahaanPas encore d'évaluation
- Radiography of Shoulder and ArmDocument81 pagesRadiography of Shoulder and ArmKristina ShresthaPas encore d'évaluation
- PERIPHERAL JOINT MOBILIZATION - Lower Limbs (1) - 052048Document34 pagesPERIPHERAL JOINT MOBILIZATION - Lower Limbs (1) - 052048MUGISHA GratienPas encore d'évaluation
- Superficial and Deep ReflexesDocument28 pagesSuperficial and Deep ReflexesShilpa SPas encore d'évaluation
- Pathophysiology Congenital Heart Disease-1Document54 pagesPathophysiology Congenital Heart Disease-1single_ladyPas encore d'évaluation
- Dasar VentilatorDocument40 pagesDasar Ventilatorsingle_ladyPas encore d'évaluation
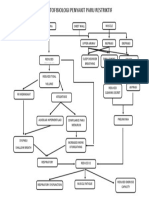
- Paru RestriktifDocument1 pageParu Restriktifsingle_ladyPas encore d'évaluation
- Patfis Valvular Heart DiseaseDocument1 pagePatfis Valvular Heart Diseasesingle_ladyPas encore d'évaluation
- Tatalaksana Rehabilitasi Penyakit Jantung BawaanDocument38 pagesTatalaksana Rehabilitasi Penyakit Jantung Bawaansingle_ladyPas encore d'évaluation
- Patfis Valvular Heart DiseaseDocument1 pagePatfis Valvular Heart Diseasesingle_ladyPas encore d'évaluation
- Pretest Kardiorespi UnaDocument60 pagesPretest Kardiorespi Unasingle_ladyPas encore d'évaluation
- Management of Acute Achilles Tendon RuptureDocument226 pagesManagement of Acute Achilles Tendon RuptureAnjatPas encore d'évaluation
- Tatalaksana Rehabilitasi Penyakit Jantung BawaanDocument38 pagesTatalaksana Rehabilitasi Penyakit Jantung Bawaansingle_ladyPas encore d'évaluation
- Collaborative Practice With Nurses in Incontinence CareDocument25 pagesCollaborative Practice With Nurses in Incontinence Caresingle_ladyPas encore d'évaluation
- Patofisiology Urinary IncontinenceDocument45 pagesPatofisiology Urinary Incontinencesingle_ladyPas encore d'évaluation
- Kinesiology ElbowDocument53 pagesKinesiology Elbowsingle_ladyPas encore d'évaluation
- Theraex For IKFRDocument130 pagesTheraex For IKFRsingle_ladyPas encore d'évaluation
- Kinesiologi Siku-Pf UnaDocument59 pagesKinesiologi Siku-Pf Unasingle_ladyPas encore d'évaluation
- Pathophysiology-Pathomechanics Dan Penegakan Diagnosis OsteoporosisDocument90 pagesPathophysiology-Pathomechanics Dan Penegakan Diagnosis Osteoporosissingle_ladyPas encore d'évaluation
- Pathophysiology-Pathomechanics Dan Penegakan Diagnosis OsteoporosisDocument90 pagesPathophysiology-Pathomechanics Dan Penegakan Diagnosis Osteoporosissingle_ladyPas encore d'évaluation
- Disorders of The Knee FebyDocument19 pagesDisorders of The Knee Febysingle_ladyPas encore d'évaluation
- Patofisiology Urinary IncontinenceDocument45 pagesPatofisiology Urinary Incontinencesingle_ladyPas encore d'évaluation
- Elbow AbnormalDocument21 pagesElbow Abnormalsingle_ladyPas encore d'évaluation
- Common Problem of HIPDocument40 pagesCommon Problem of HIPsingle_ladyPas encore d'évaluation
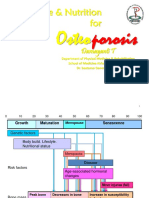
- Exercise Nutrition N OsteoporosisDocument73 pagesExercise Nutrition N Osteoporosissingle_ladyPas encore d'évaluation
- Disorders of The Knee FebyDocument19 pagesDisorders of The Knee Febysingle_ladyPas encore d'évaluation
- Case Pediatri Cerebral PalsyDocument20 pagesCase Pediatri Cerebral Palsysingle_ladyPas encore d'évaluation
- Case Report IdentityDocument16 pagesCase Report Identitysingle_ladyPas encore d'évaluation
- Short Case II: Jufri Febrianto, MDDocument16 pagesShort Case II: Jufri Febrianto, MDsingle_ladyPas encore d'évaluation
- Splinting: Darsuna Mardhiah Dr. Tertianto Prabowo, SP - KFRDocument79 pagesSplinting: Darsuna Mardhiah Dr. Tertianto Prabowo, SP - KFRsingle_ladyPas encore d'évaluation
- Delchev Alexander - The Modern Reti An Anti-Slav Repertoire 2012-OCR ChessStars 214pDocument214 pagesDelchev Alexander - The Modern Reti An Anti-Slav Repertoire 2012-OCR ChessStars 214pVicalo Alonso100% (1)
- Ambush Squad RecordDocument1 pageAmbush Squad RecordLudo WhooPas encore d'évaluation
- Bones and SkeletonsDocument17 pagesBones and SkeletonsMr ReasonPas encore d'évaluation
- Alize EZ Criss Cross Baby Blanket in Bernat Downloadable PDF 2Document2 pagesAlize EZ Criss Cross Baby Blanket in Bernat Downloadable PDF 2adinaPas encore d'évaluation
- Muscle: ScienceDocument161 pagesMuscle: ScienceAlessandro ValentimPas encore d'évaluation
- ATN Performance ListDocument10 pagesATN Performance ListCory Mull0% (1)
- Big Waaagh Magic CardsDocument2 pagesBig Waaagh Magic Cardsjdwratcliffe8552Pas encore d'évaluation
- STD 3 GK-49-74Document30 pagesSTD 3 GK-49-74lambajituPas encore d'évaluation
- Mikonosuke KawaishiDocument1 pageMikonosuke KawaishiOmar ContrerasPas encore d'évaluation
- Conditioning Method RecapDocument7 pagesConditioning Method RecaphmimezPas encore d'évaluation
- World Class Revision ExercisesDocument3 pagesWorld Class Revision ExercisesNivia MartinezPas encore d'évaluation
- THE ELDER SCROLLS - Oblivion - GuideDocument330 pagesTHE ELDER SCROLLS - Oblivion - GuideMelanieReyesPas encore d'évaluation
- Reman-C10508567 Caterpillar RemanDocument32 pagesReman-C10508567 Caterpillar RemanElmer Lagua Malpaso67% (3)
- Jokertrike TopoľčanyDocument4 pagesJokertrike TopoľčanyIvan Gonzo Sabo100% (1)
- Pile Design SpreadsheetDocument180 pagesPile Design SpreadsheetSharookhan ShajahanPas encore d'évaluation
- Alekhine With 4.a4 PDFDocument16 pagesAlekhine With 4.a4 PDFrubenkeller5204Pas encore d'évaluation
- 50H - 50MDocument437 pages50H - 50MFran Chaf100% (1)
- Test LOAD OKDocument3 pagesTest LOAD OKdaniel aprio juremiPas encore d'évaluation
- Mortal Kombat Finish Him Font - Google SearchDocument1 pageMortal Kombat Finish Him Font - Google SearchDouglas LemusPas encore d'évaluation
- PSDA Rescue Swimmer Program 1 & 2Document4 pagesPSDA Rescue Swimmer Program 1 & 2matthew6056Pas encore d'évaluation
- Kinesiology PDFDocument12 pagesKinesiology PDFDharamvir PrajapatiPas encore d'évaluation
- Examen Final - Semana 8 - ESP - SEGUNDO BLOQUE-INGLES GENERAL II - (GRUPO2)Document16 pagesExamen Final - Semana 8 - ESP - SEGUNDO BLOQUE-INGLES GENERAL II - (GRUPO2)Alex AlegriaPas encore d'évaluation
- MARATHON - 5 Hour - 6 Month Training ProgramDocument1 pageMARATHON - 5 Hour - 6 Month Training ProgrammiroswatPas encore d'évaluation
- Rolemaster Skill SheetDocument1 pageRolemaster Skill SheetwolsePas encore d'évaluation
- CRPG Book 2.0-1Document529 pagesCRPG Book 2.0-1Bruno Siffredi100% (4)
- Dumbbell Workout Routine FinalDocument18 pagesDumbbell Workout Routine FinalSachith SeneviratnaPas encore d'évaluation
- NC ResumeDocument3 pagesNC Resumeapi-139535983Pas encore d'évaluation
- Question Tags - Essay TaskDocument1 pageQuestion Tags - Essay TaskHidayatul HikmahPas encore d'évaluation
- Math10 - NeyDocument4 pagesMath10 - NeyAlbert Dar LinisPas encore d'évaluation
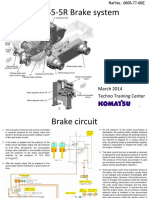
- GD755-5R 06 Brake SystemDocument22 pagesGD755-5R 06 Brake Systemyongki fcPas encore d'évaluation