Vous aimerez peut-être aussi
- Interaksi FarmakokinetikDocument43 pagesInteraksi FarmakokinetikGarry B GunawanPas encore d'évaluation
- 1 Drug Interaction Spring 2024Document68 pages1 Drug Interaction Spring 2024192315Pas encore d'évaluation
- Drug InteractionDocument23 pagesDrug Interactionsinghjsanjay885Pas encore d'évaluation
- Drug Interactions: Vivian Soetikno Department of Pharmacology & Therapeutics, FmuiDocument53 pagesDrug Interactions: Vivian Soetikno Department of Pharmacology & Therapeutics, FmuiAciPas encore d'évaluation
- Drug InteractionDocument36 pagesDrug Interaction101 102100% (1)
- Drug Interactions: DR - Omer A.A.S. Rikaby BSC Pharmacy MSC Clinical Pharmacy MbaDocument40 pagesDrug Interactions: DR - Omer A.A.S. Rikaby BSC Pharmacy MSC Clinical Pharmacy MbaAbdalla Kazzam100% (1)
- Drugs Interaction: DR - Datten Bangun MSC, SPFK & DR - Dr.Tri Widyawati MSCDocument39 pagesDrugs Interaction: DR - Datten Bangun MSC, SPFK & DR - Dr.Tri Widyawati MSCpsyPas encore d'évaluation
- Drug InteractionDocument77 pagesDrug InteractionAthirah Muhammad NoerPas encore d'évaluation
- Irsan-Drug Interaction 2020Document65 pagesIrsan-Drug Interaction 2020Bayu WisnuPas encore d'évaluation
- 2 Drug Interaction Introduction YogiartoDocument23 pages2 Drug Interaction Introduction YogiartoPebby AnggerainiPas encore d'évaluation
- IVMS Pharmacokinetics Drug Elimination 2Document33 pagesIVMS Pharmacokinetics Drug Elimination 2piinyPas encore d'évaluation
- Sunitha - Drug InteractionsDocument49 pagesSunitha - Drug InteractionsSunitha Katta100% (1)
- Kuliah-Geriatri FarmakoDocument60 pagesKuliah-Geriatri FarmakoTenta Hartian HendyatamaPas encore d'évaluation
- Interaksi Obat - Farmakologi AfifahDocument42 pagesInteraksi Obat - Farmakologi AfifahShaPas encore d'évaluation
- Drug Interaction 2Document65 pagesDrug Interaction 2alhader libraryPas encore d'évaluation
- Drug InteractionsDocument18 pagesDrug InteractionsAnoosha FarooquiPas encore d'évaluation
- 6 Robertson - Clinical Drug Interactions - 0Document44 pages6 Robertson - Clinical Drug Interactions - 0Piyush BandelaPas encore d'évaluation
- Presented By: Raghav Dogra M.Pharm (Analysis) 2016-2017Document38 pagesPresented By: Raghav Dogra M.Pharm (Analysis) 2016-2017gggPas encore d'évaluation
- DMC FinalsDocument64 pagesDMC Finalskaye agustinPas encore d'évaluation
- Drug InteractionDocument27 pagesDrug InteractionRida Nur RafidahPas encore d'évaluation
- 16 - Metabolism and Pharmacogenomics - 2023Document29 pages16 - Metabolism and Pharmacogenomics - 2023Rhythm BhardwajPas encore d'évaluation
- Drugs Interactions May 2010Document28 pagesDrugs Interactions May 2010Michael MohammedPas encore d'évaluation
- New General PharmacologyDocument85 pagesNew General PharmacologyOfkala TarikuPas encore d'évaluation
- Drug Interactions: New Zealand College of PharmacistsDocument34 pagesDrug Interactions: New Zealand College of PharmacistsTarek HusseinPas encore d'évaluation
- Drug Interaction and Adverse Drug Interactions PCI StudentsDocument38 pagesDrug Interaction and Adverse Drug Interactions PCI Studentsabdijorgi1Pas encore d'évaluation
- CU SHAH - Refresher Course - 02-10-2016 FinalDocument38 pagesCU SHAH - Refresher Course - 02-10-2016 FinalParthMairPas encore d'évaluation
- Drug InteractonsDocument32 pagesDrug InteractonsHarun MohamedPas encore d'évaluation
- 1-2 Introduccion and PharmacokineticDocument28 pages1-2 Introduccion and PharmacokineticMewael TesfamichaelPas encore d'évaluation
- Principle of PharmacologyDocument40 pagesPrinciple of PharmacologySolaPas encore d'évaluation
- 12 Drug Interactions 2012-2013 Penzak 3Document15 pages12 Drug Interactions 2012-2013 Penzak 3QuangvodsPas encore d'évaluation
- Drug Interactions: Endang Windiastuti, Dr.,Spa (K) Satgas Farmasi IdaiDocument30 pagesDrug Interactions: Endang Windiastuti, Dr.,Spa (K) Satgas Farmasi IdaiFredik MaloPas encore d'évaluation
- Ilmu Resep 1 - Drug Interaction1 2017Document41 pagesIlmu Resep 1 - Drug Interaction1 2017NatanaelHendrySantosoPas encore d'évaluation
- MDW 2017 Day 2 Track 2 Session 9 Bradley Reducing PolypharmacyDocument9 pagesMDW 2017 Day 2 Track 2 Session 9 Bradley Reducing PolypharmacyAmparo VillamilPas encore d'évaluation
- Wk7 FunMed - 4. PK (ADME2) DR MalekigorjiDocument44 pagesWk7 FunMed - 4. PK (ADME2) DR MalekigorjiziaduddinPas encore d'évaluation
- 15 GMppt-chapter18-2020 (Ok)Document19 pages15 GMppt-chapter18-2020 (Ok)Kw ChanPas encore d'évaluation
- Protein Binding of DrugsDocument29 pagesProtein Binding of Drugstry.vishaldhamole78Pas encore d'évaluation
- Drug Interaction Can Be Defined As TheDocument34 pagesDrug Interaction Can Be Defined As TheIstianah Es100% (1)
- 1 Farmakogenomik 2023Document51 pages1 Farmakogenomik 2023yayu latifahPas encore d'évaluation
- Drug Interactions: DR Michelle Munyoro MBCHB, MCPH (Uz) 6 February 2019Document32 pagesDrug Interactions: DR Michelle Munyoro MBCHB, MCPH (Uz) 6 February 2019Stanley Tatenda MukonoPas encore d'évaluation
- Kuliah Drug Interactions and ADRDocument88 pagesKuliah Drug Interactions and ADRAnda DarmayantiPas encore d'évaluation
- Drug Interaction in Dentistry: Dr. Benjamin ZeitlinDocument15 pagesDrug Interaction in Dentistry: Dr. Benjamin ZeitlinJack PaiPas encore d'évaluation
- PharmacogenomicsDocument56 pagesPharmacogenomicsapi-650133203Pas encore d'évaluation
- Drug Induce Liver InjuryDocument77 pagesDrug Induce Liver InjuryReyhan Prayogo100% (1)
- Drug Interaction 2Document28 pagesDrug Interaction 2Dixit LanghnejaPas encore d'évaluation
- Drug InteractionDocument24 pagesDrug InteractionChuol Mateat KanPas encore d'évaluation
- Drug-Drug InteractionDocument9 pagesDrug-Drug InteractionHo Shi XianPas encore d'évaluation
- Drug InterractionsDocument15 pagesDrug InterractionsYIKI ISAACPas encore d'évaluation
- Ios g56fBJEDfmJmkl6UDocument207 pagesIos g56fBJEDfmJmkl6UBawan ZahirPas encore d'évaluation
- Drug InteractionsDocument5 pagesDrug Interactionsvajkember100% (1)
- Pharmacokinetic Drug InteractionsDocument3 pagesPharmacokinetic Drug InteractionsRaghu RamarapuPas encore d'évaluation
- INTRODUCTION TO DRUG INTERACTIONS-PHA 303 - DR Ogunleye - 1Document20 pagesINTRODUCTION TO DRUG INTERACTIONS-PHA 303 - DR Ogunleye - 1Ebenezer SamuelPas encore d'évaluation
- Drug InteractionsDocument26 pagesDrug InteractionsMahum SohailPas encore d'évaluation
- General Pharmacology For MD Medicine/ Selection Exam: Chamila MettanandaDocument70 pagesGeneral Pharmacology For MD Medicine/ Selection Exam: Chamila MettanandaThanushan BalasingamPas encore d'évaluation
- Presentation2 130918234532 Phpapp01Document59 pagesPresentation2 130918234532 Phpapp01Julius Kent QuilapioPas encore d'évaluation
- Pharmacokinetic Interaction: DR - Datten Bangun MSC, SPFK & DR - Zulkarnain RangkutyDocument39 pagesPharmacokinetic Interaction: DR - Datten Bangun MSC, SPFK & DR - Zulkarnain RangkutyCatherine ElizabetPas encore d'évaluation
- Drug Interaction-SibyDocument93 pagesDrug Interaction-SibyAswin DamodaranPas encore d'évaluation
- Protein Drug Binding: By: Kishan Arudra M.PharmDocument21 pagesProtein Drug Binding: By: Kishan Arudra M.PharmGianniPas encore d'évaluation
- Handbook of Drug Interaction and the Mechanism of InteractionD'EverandHandbook of Drug Interaction and the Mechanism of InteractionÉvaluation : 1 sur 5 étoiles1/5 (1)
- SkeliosisDocument55 pagesSkeliosisevelynPas encore d'évaluation
- Ya Ya YaDocument10 pagesYa Ya YaevelynPas encore d'évaluation
- Science Program in Public Health STIKES Payung Negeri PekanbaruDocument3 pagesScience Program in Public Health STIKES Payung Negeri PekanbaruevelynPas encore d'évaluation
- Shoulder Anatomy Tcm396-166103Document17 pagesShoulder Anatomy Tcm396-166103evelynPas encore d'évaluation
- Anatomy ShoulderDocument37 pagesAnatomy ShoulderevelynPas encore d'évaluation
- Book Eyelid Tumor)Document288 pagesBook Eyelid Tumor)evelyn100% (1)
- How To Measure ZincDocument4 pagesHow To Measure ZincevelynPas encore d'évaluation
- Daftar DDDDocument6 pagesDaftar DDDelisemilPas encore d'évaluation
- INDICATIIDocument17 pagesINDICATIITarek TarekPas encore d'évaluation
- Medication Administration: BY Thomas PetriciniDocument204 pagesMedication Administration: BY Thomas PetricinisaheedvkPas encore d'évaluation
- Drug InterationsDocument5 pagesDrug InterationsAsmaa RadwanPas encore d'évaluation
- Chiral PharmacologyDocument33 pagesChiral Pharmacologysar86100% (1)
- A Review On Supac Guidance For Modified Release Solid Oraldosage FormsDocument9 pagesA Review On Supac Guidance For Modified Release Solid Oraldosage FormsAhmad Al-RusasiPas encore d'évaluation
- Pharmaceutical Side Effects Google SquareDocument267 pagesPharmaceutical Side Effects Google SquareCharlie HarePas encore d'évaluation
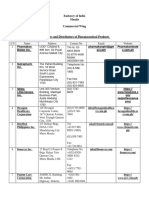
- Importers of Pharmaceutical Products in PHDocument12 pagesImporters of Pharmaceutical Products in PHmarketing lakshPas encore d'évaluation
- Avamys 1Document27 pagesAvamys 1girishtrivediPas encore d'évaluation
- Pharmacology ADMEDocument27 pagesPharmacology ADMENguyen HuyPas encore d'évaluation
- 0.1.clinical PharmacokineticsDocument60 pages0.1.clinical PharmacokineticsSolomon D FatormaPas encore d'évaluation
- Bpharma RCRVDocument4 pagesBpharma RCRVAshok EerlaPas encore d'évaluation
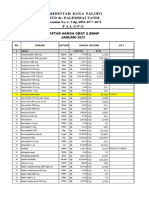
- Daftar Harga 2023Document94 pagesDaftar Harga 2023setiawan100% (1)
- Introduction To PharmacologyDocument30 pagesIntroduction To PharmacologyCandy crush100% (1)
- Director of Pharmacy, Clinical PharmacistDocument3 pagesDirector of Pharmacy, Clinical Pharmacistapi-77860855Pas encore d'évaluation
- Pharmacology Toxicology - 4th EdDocument41 pagesPharmacology Toxicology - 4th EdYorlenie Juárez100% (1)
- 2 Ndpaper 1Document7 pages2 Ndpaper 1Shahid NoorPas encore d'évaluation
- Bioequivalence of Two Pregabalin 300 MG Capsules (Neurexal and Lyrica) in Healthy Human VolunteersDocument5 pagesBioequivalence of Two Pregabalin 300 MG Capsules (Neurexal and Lyrica) in Healthy Human VolunteerscaturPas encore d'évaluation
- OBATDocument61 pagesOBATptgraha mitraPas encore d'évaluation
- Introduction To Drug InteractionsDocument19 pagesIntroduction To Drug InteractionsPyara MunnaPas encore d'évaluation
- Indo Africa Indianparticipants-09Document14 pagesIndo Africa Indianparticipants-09Brinda ReddyPas encore d'évaluation
- Pharmacology Notes: Learning OutcomesDocument22 pagesPharmacology Notes: Learning OutcomesHarlene Joyce ReyPas encore d'évaluation
- Fundamental Concepts of PharmacologyDocument5 pagesFundamental Concepts of PharmacologyphoebePas encore d'évaluation
- Daftar Obat-Obatan Rumah Sakit AzzahraDocument12 pagesDaftar Obat-Obatan Rumah Sakit Azzahraelimawati elimawatiPas encore d'évaluation
- Book 2Document9 pagesBook 2Aditya PamungkasPas encore d'évaluation
- Tablas de Dosificacion Kirk 9na EdDocument68 pagesTablas de Dosificacion Kirk 9na EdMarlieth Rosales HernandezPas encore d'évaluation
- Criteria # Efficacy Points + + + +: Doltegravir/Abaravir/LamividuneDocument5 pagesCriteria # Efficacy Points + + + +: Doltegravir/Abaravir/LamividuneValerie Gonzaga-CarandangPas encore d'évaluation
- St. John's Wort: Clinical OverviewDocument14 pagesSt. John's Wort: Clinical OverviewTrismegistePas encore d'évaluation
- Jetlax's CNS Pharmacology Cheat Sheet For The Philippines v6.0 at Bit - Ly - CNSPcol - See Bit - Ly - CNSHandouts For 5.0 CorrectionsDocument61 pagesJetlax's CNS Pharmacology Cheat Sheet For The Philippines v6.0 at Bit - Ly - CNSPcol - See Bit - Ly - CNSHandouts For 5.0 CorrectionsShalimar BasmanPas encore d'évaluation
- Formularium RS 2022Document76 pagesFormularium RS 2022Boy ReynaldiPas encore d'évaluation