Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Rising Syphilis Rates in Pregnant WomenDocument34 pagesRising Syphilis Rates in Pregnant Womenlalee704Pas encore d'évaluation
- Algorithm MkacsDocument1 pageAlgorithm MkacsKrystel SesePas encore d'évaluation
- Quiz History - Assessment OneDocument9 pagesQuiz History - Assessment OneDibyendu KarmakarPas encore d'évaluation
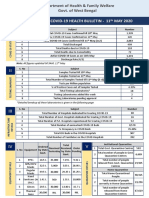
- West Bengal COVID-19 health bulletin updatesDocument4 pagesWest Bengal COVID-19 health bulletin updatesSoham SarangiPas encore d'évaluation
- The Difference Between HIV and AidsDocument14 pagesThe Difference Between HIV and AidsAnonymous bq4KY0mcWGPas encore d'évaluation
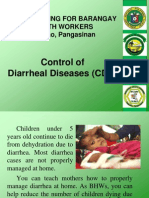
- CDD Training for BHWs in CalasiaoDocument18 pagesCDD Training for BHWs in Calasiao700AIDANPas encore d'évaluation
- Plasmodium Malariae: Parasite and Disease: William E. Collins and Geoffrey M. JefferyDocument14 pagesPlasmodium Malariae: Parasite and Disease: William E. Collins and Geoffrey M. JefferyReynaldi FirmansyahPas encore d'évaluation
- Prevalence and Antibiotic Resistance of Staphylococcus aureus in a Pakistani HospitalDocument4 pagesPrevalence and Antibiotic Resistance of Staphylococcus aureus in a Pakistani Hospitalzia ul RahmanPas encore d'évaluation
- Httpslms - Naco.gov - Infrontendcontentnational Guidelines For PPTCT PDFDocument137 pagesHttpslms - Naco.gov - Infrontendcontentnational Guidelines For PPTCT PDFshlok jainPas encore d'évaluation
- What Is Typhoid FeverDocument5 pagesWhat Is Typhoid FeverKameh Dani Adrian Wadzon'sPas encore d'évaluation
- Hubungan Pengetahuan Terhadap Perilaku Penggunaan Suplemen Kesehatan DIMASA COVID192020Document6 pagesHubungan Pengetahuan Terhadap Perilaku Penggunaan Suplemen Kesehatan DIMASA COVID192020nur halimaPas encore d'évaluation
- Article in Press: Florence Nightingale's Environmental Theory and Its in Uence On Contemporary Infection ControlDocument8 pagesArticle in Press: Florence Nightingale's Environmental Theory and Its in Uence On Contemporary Infection ControlBalqist Asyawa Andra PutriPas encore d'évaluation
- Scabies DialogDocument2 pagesScabies DialogMurdiyani Nina AgustinaPas encore d'évaluation
- Kumpulan Soal NCLEX Dengan Jawaban Dan PembahasanDocument7 pagesKumpulan Soal NCLEX Dengan Jawaban Dan PembahasanjunitanjunPas encore d'évaluation
- Drug Study Tetanus ToxoidDocument1 pageDrug Study Tetanus ToxoidBunnie Alpha100% (3)
- Samenvatting Infectie en InflammatieDocument169 pagesSamenvatting Infectie en InflammatiejeskevandiemenPas encore d'évaluation
- Acute Upper Respiratory Tract Infection. 1Document20 pagesAcute Upper Respiratory Tract Infection. 1Joana Carolina QuiambaoPas encore d'évaluation
- UTI - Concept MapDocument1 pageUTI - Concept MapZam Pamate50% (2)
- Genital Ulcer DiseaseDocument29 pagesGenital Ulcer DiseaseFu' BudhyPas encore d'évaluation
- LB 1 Master XXXXDocument2 250 pagesLB 1 Master XXXXRisa de ApnaPas encore d'évaluation
- Human Nocardia Infections: A Review of Pulmonary NocardiosisDocument7 pagesHuman Nocardia Infections: A Review of Pulmonary NocardiosisAyu Nurislami WulandariPas encore d'évaluation
- Protozoa Plasmodium Causes MalariaDocument22 pagesProtozoa Plasmodium Causes MalariaMalkhatibPas encore d'évaluation
- Biology Class 12 ProjectDocument26 pagesBiology Class 12 ProjectZinzekoPas encore d'évaluation
- ScabiesDocument38 pagesScabiesSiti Sabrina AtamiaPas encore d'évaluation
- Definition of TermsDocument29 pagesDefinition of TermsJohn Henry G. Gabriel IV100% (6)
- ImmunizationDocument1 pageImmunizationMicah Lou CalambaPas encore d'évaluation
- Urinary Tract Infections (UTI)Document25 pagesUrinary Tract Infections (UTI)microperadeniya0% (1)
- Penyuluhan Pencegahan Penyakit Tuberkulosis (TBC) Era New NormalDocument8 pagesPenyuluhan Pencegahan Penyakit Tuberkulosis (TBC) Era New NormalTrihandi PamungkasPas encore d'évaluation
- Anti-Spitting Ordinance of MagsaysayDocument2 pagesAnti-Spitting Ordinance of MagsaysayAlfredo BaulaPas encore d'évaluation
- Mastigophora TableDocument1 pageMastigophora TableJoshua TrinidadPas encore d'évaluation