Vous aimerez peut-être aussi
- European Consensus On The Management of RDSDocument41 pagesEuropean Consensus On The Management of RDSDeddy Supriyadi100% (1)
- Surfactant-Administration ODN v2 150418Document11 pagesSurfactant-Administration ODN v2 150418Deep AdhikariPas encore d'évaluation
- BRONCHOPULMONARY DYSPLASIA ModifiedDocument48 pagesBRONCHOPULMONARY DYSPLASIA ModifiedajanmjPas encore d'évaluation
- COVID-19 Management of Critical Care Cases PDFDocument6 pagesCOVID-19 Management of Critical Care Cases PDFLubna AliPas encore d'évaluation
- Guidelines For Surfactant Administration (Surfactant Replacement Therapy) University of Iowa Stead Family Children's Hospital 2Document1 pageGuidelines For Surfactant Administration (Surfactant Replacement Therapy) University of Iowa Stead Family Children's Hospital 2Anonymous 18GsyXbPas encore d'évaluation
- Surfactant Final 2Document5 pagesSurfactant Final 2anuPas encore d'évaluation
- Guideline For The Prevention of Bronchopulmonary Dysplasia and Assessment of Evolving BPDDocument28 pagesGuideline For The Prevention of Bronchopulmonary Dysplasia and Assessment of Evolving BPDjanfk2000Pas encore d'évaluation
- HFNC Guidelines AustraliaDocument13 pagesHFNC Guidelines AustraliaMASIEL AMELIA BARRANTES ARCEPas encore d'évaluation
- Chronic Lung DiseaseDocument59 pagesChronic Lung DiseaseSitaPas encore d'évaluation
- Surfactant Replacement Therapy - 2019Document8 pagesSurfactant Replacement Therapy - 2019Saravanan Nallasivan100% (2)
- SurvantaDocument2 pagesSurvantasyafiraPas encore d'évaluation
- FINAL COVID19 1 April 2021Document14 pagesFINAL COVID19 1 April 2021Wleed KhledPas encore d'évaluation
- Respiratory Distress Syndrome, Transient Tachypnea of The Newborn and Meconium Aspiration SyndromeDocument69 pagesRespiratory Distress Syndrome, Transient Tachypnea of The Newborn and Meconium Aspiration SyndromeKate PanoliPas encore d'évaluation
- Zgddekzz 23 11 1097Document6 pagesZgddekzz 23 11 1097arieza nur pratamaPas encore d'évaluation
- Nasal IMV - Gatot PDFDocument43 pagesNasal IMV - Gatot PDFtutiarlyPas encore d'évaluation
- Respiratory Distress SyndromeDocument54 pagesRespiratory Distress SyndromeKristine CaringalPas encore d'évaluation
- Efficacy of Non-Invasive Respiratory Support Modes For Primary Respiratory Support in Preterm Neonates With Respiratory Distress Syndrome Systematic Review and Network Meta-AnalysisDocument24 pagesEfficacy of Non-Invasive Respiratory Support Modes For Primary Respiratory Support in Preterm Neonates With Respiratory Distress Syndrome Systematic Review and Network Meta-Analysisalan tomePas encore d'évaluation
- Nebulized Surfactant To Reduce Severity of Respiratory Distress: A Blinded Parallel, Randomized Controlled TrialDocument36 pagesNebulized Surfactant To Reduce Severity of Respiratory Distress: A Blinded Parallel, Randomized Controlled TrialRachelle Celina AlmontePas encore d'évaluation
- Effect of T-Piece Resuscitator Versus Self Inflating Bag On Arterial CO Levels in Preterm NeonatesDocument8 pagesEffect of T-Piece Resuscitator Versus Self Inflating Bag On Arterial CO Levels in Preterm NeonatesRaja SekarPas encore d'évaluation
- UntitledDocument24 pagesUntitledBella FebriantiPas encore d'évaluation
- Nippv Revisi Final Picu Nicu MaretDocument51 pagesNippv Revisi Final Picu Nicu MaretJulian Ammar Zaidan GunawanPas encore d'évaluation
- Difficult Weaning in COVID 19Document53 pagesDifficult Weaning in COVID 19rkapatworkPas encore d'évaluation
- Terapi Oxygen Pada Pasien Covd-19Document24 pagesTerapi Oxygen Pada Pasien Covd-19normamPas encore d'évaluation
- RSI ResidentDocument58 pagesRSI ResidentHidayati IdaPas encore d'évaluation
- ICU Management of COVID Patients: PreventionDocument13 pagesICU Management of COVID Patients: PreventionYuri SadewoPas encore d'évaluation
- Journal ClubDocument39 pagesJournal Clubgpediatrics myPas encore d'évaluation
- ITISMITA Biswal MSC, Nursing 2 YearDocument48 pagesITISMITA Biswal MSC, Nursing 2 YearGandimareiPas encore d'évaluation
- Ventilator: Associated Pneumonia (VAP)Document36 pagesVentilator: Associated Pneumonia (VAP)D. Melba S.S ChinnaPas encore d'évaluation
- COVID 19. 4 - 13 KashmerDocument42 pagesCOVID 19. 4 - 13 KashmerIshfaq GanaiPas encore d'évaluation
- Guidelines For Surfactant AdministrationDocument4 pagesGuidelines For Surfactant AdministrationDella Elvina RoeslandPas encore d'évaluation
- Hyaline Membrane Disease 3Document2 pagesHyaline Membrane Disease 3UgaugaaPas encore d'évaluation
- Directorate General of Health Services, Mohfw, Goi Comprehensive Guidelines For Management of Covid-19 Patients Asymptomatic Mild Moderate SevereDocument2 pagesDirectorate General of Health Services, Mohfw, Goi Comprehensive Guidelines For Management of Covid-19 Patients Asymptomatic Mild Moderate SevereSpecial OPD SVMCHRCPas encore d'évaluation
- Niv HFNCDocument15 pagesNiv HFNCFrank VaronaPas encore d'évaluation
- Journal Club: PRESENTOR: Dr. Pranaya Mall MODERATOR:. Dr. Pratima (Asst. Prof.)Document53 pagesJournal Club: PRESENTOR: Dr. Pranaya Mall MODERATOR:. Dr. Pratima (Asst. Prof.)Pranay MallPas encore d'évaluation
- Surf Act Ant ReplacementDocument28 pagesSurf Act Ant Replacementapi-27504339100% (3)
- TivaDocument38 pagesTivasunny kumar100% (1)
- Sudeshna Banerjee M.SC (N) 2 Year HfconDocument30 pagesSudeshna Banerjee M.SC (N) 2 Year HfconSanjay Kumar Sanju100% (1)
- Jurnal Pubme 1 RdsDocument13 pagesJurnal Pubme 1 Rdsriri risna aPas encore d'évaluation
- Vincent Brody Care PlanDocument10 pagesVincent Brody Care PlanKarina Rodriguez50% (2)
- AIIMS Issues New Guidelines For Treatment of CovidDocument7 pagesAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarPas encore d'évaluation
- Weaning ProtocolDocument6 pagesWeaning ProtocolerwanPas encore d'évaluation
- TreatmentProtocol 10-4-2021Document3 pagesTreatmentProtocol 10-4-2021Anishk SinghPas encore d'évaluation
- COVID-19 Drug TherapyDocument44 pagesCOVID-19 Drug Therapyshams43Pas encore d'évaluation
- Pneumonia: Tim Teaching Farmakoterapi Penyakit Infeksi Dan Keganasan Fakultas Farmasi Universitas Jember Gasal 20211Document67 pagesPneumonia: Tim Teaching Farmakoterapi Penyakit Infeksi Dan Keganasan Fakultas Farmasi Universitas Jember Gasal 20211Evie WulansariPas encore d'évaluation
- AIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)Document7 pagesAIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)senthil kumarPas encore d'évaluation
- Spontaneous Awakening Trial PDFDocument1 pageSpontaneous Awakening Trial PDFyonoPas encore d'évaluation
- Postanesthesia Care: Dhany BudipratamaDocument36 pagesPostanesthesia Care: Dhany BudipratamaAbu Bakr Ar RaziPas encore d'évaluation
- Randomized Trial of Laryngeal Mask Airway Versus Endotracheal Intubation For Surfactant DeliveryDocument6 pagesRandomized Trial of Laryngeal Mask Airway Versus Endotracheal Intubation For Surfactant DeliveryKelompok 8 PF HTTPas encore d'évaluation
- Hospital-Acquired Pneumonia (HAP) & Ventilator-Associated Pneumonia (VAP) Healthcare-Associated Pneumonia (HCAP)Document32 pagesHospital-Acquired Pneumonia (HAP) & Ventilator-Associated Pneumonia (VAP) Healthcare-Associated Pneumonia (HCAP)Kamel HadyPas encore d'évaluation
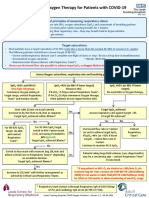
- Guidance On Oxygen Therapy For Patients With COVID-19: General Principles of Assessing Respiratory StatusDocument1 pageGuidance On Oxygen Therapy For Patients With COVID-19: General Principles of Assessing Respiratory StatusAsh mohamedPas encore d'évaluation
- Surfactant Replacement Therapy in Neonates-NNFI CPG Dec2021Document48 pagesSurfactant Replacement Therapy in Neonates-NNFI CPG Dec2021Preethi R BhatPas encore d'évaluation
- Covid 19 Aerosol Generating ProceduresDocument4 pagesCovid 19 Aerosol Generating ProceduresAhmed Ben BellaPas encore d'évaluation
- Mechanical Ventilation in NeonatesDocument60 pagesMechanical Ventilation in NeonatesZuhair Aldajani زهير عمر الدجاني100% (3)
- Non Invasive Ventilation - DR RinaDocument76 pagesNon Invasive Ventilation - DR RinaTitik sukamtiPas encore d'évaluation
- CPG BronchiolitisDocument4 pagesCPG BronchiolitisLouis SudarioPas encore d'évaluation
- Application HFOV in NICU - Lily RundjanDocument43 pagesApplication HFOV in NICU - Lily Rundjandiah ayu pitalokaPas encore d'évaluation
- Best Practice of Pneumonia Management in Pandemic Era: Retno Asih SetyoningrumDocument48 pagesBest Practice of Pneumonia Management in Pandemic Era: Retno Asih SetyoningrumNurul aina MardhiyahPas encore d'évaluation
- Riesgo Alto de Manejo de La Vía AereaDocument17 pagesRiesgo Alto de Manejo de La Vía AereaAntonio AlonsoPas encore d'évaluation
- Lung Ultrasound Score As A Predictor of Ventilator Use in Preterm Infants With Dyspnea Within 24 H After Dhospitalization PDFDocument8 pagesLung Ultrasound Score As A Predictor of Ventilator Use in Preterm Infants With Dyspnea Within 24 H After Dhospitalization PDFcesar juarezPas encore d'évaluation
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideD'EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuidePas encore d'évaluation
- Aulia Putri - Case SNNTDocument29 pagesAulia Putri - Case SNNTAulia P NurjannahPas encore d'évaluation
- CTG Interpretation of CTG and CFHM During Antepartum and Intrapartum Periods Ho Lai FongDocument33 pagesCTG Interpretation of CTG and CFHM During Antepartum and Intrapartum Periods Ho Lai FongSabrina AzizPas encore d'évaluation
- Waist and Hip Circumferences and Waist-Hip Ratio I-2Document1 pageWaist and Hip Circumferences and Waist-Hip Ratio I-2VenkatPas encore d'évaluation
- C A U U U T I O N: Viruses and BacteriaDocument1 pageC A U U U T I O N: Viruses and BacteriaIrish Eunice FelixPas encore d'évaluation
- Riane Pamintuan - Short StoryDocument2 pagesRiane Pamintuan - Short StoryRiane Venice PamintuanPas encore d'évaluation
- The National Guidelines For The Management of STIDocument53 pagesThe National Guidelines For The Management of STImehPas encore d'évaluation
- Patients ChartDocument1 pagePatients ChartLovely HackeyPas encore d'évaluation
- Gastroparesis in Adults Oral Erythromycin PDF 54116458939430341Document29 pagesGastroparesis in Adults Oral Erythromycin PDF 54116458939430341Rasangi Sumudu Clare SuraweeraPas encore d'évaluation
- Ethnomedicinal Uses, Phytochemistry and Pharmacological Aspects of The Genus Premna: A ReviewDocument26 pagesEthnomedicinal Uses, Phytochemistry and Pharmacological Aspects of The Genus Premna: A ReviewDavids MarinPas encore d'évaluation
- VarshaphalDocument9 pagesVarshaphalAshishh ChoprraPas encore d'évaluation
- GH 13 617Document3 pagesGH 13 617Eunice KundimanPas encore d'évaluation
- Case PresentationDocument19 pagesCase PresentationSneha PrakashPas encore d'évaluation
- All You Need To Know About Antibiotics: Tariq A. Madani, MBBS, FRCPCDocument89 pagesAll You Need To Know About Antibiotics: Tariq A. Madani, MBBS, FRCPCMansour AltalhiPas encore d'évaluation
- Full Download Ebook PDF Nursing Care Plans Diagnoses Interventions and Outcomes 9th Edition PDFDocument41 pagesFull Download Ebook PDF Nursing Care Plans Diagnoses Interventions and Outcomes 9th Edition PDFsharon.henry95197% (32)
- Cupping Therapy ChineseDocument24 pagesCupping Therapy Chinesemfabdullah100% (1)
- Feelings Inventory 0Document2 pagesFeelings Inventory 0api-292135937Pas encore d'évaluation
- Vaja RamDocument2 pagesVaja RamJitendra MalviyaPas encore d'évaluation
- Art - Atraumatic Restorative Treatment in DentistryDocument32 pagesArt - Atraumatic Restorative Treatment in DentistryPuneet ChoudharyPas encore d'évaluation
- WICM Viva LW Ischaemic BowelDocument3 pagesWICM Viva LW Ischaemic BowelisytordaPas encore d'évaluation
- IMNCIDocument13 pagesIMNCIJayalakshmiullasPas encore d'évaluation
- UntitledDocument135 pagesUntitledDr.younes95 RekaaneyPas encore d'évaluation
- Traveler's Diarrhea Treatment FlowchartDocument1 pageTraveler's Diarrhea Treatment FlowchartjaunisPas encore d'évaluation
- Traditional African MedicineDocument13 pagesTraditional African MedicineCarey G.100% (3)
- The Visa ScoreDocument2 pagesThe Visa ScoreAdmirPas encore d'évaluation
- Client - Assessment - Record vw430vDocument11 pagesClient - Assessment - Record vw430vjulianPas encore d'évaluation
- How Physical Activity Boosts Your Overall HealthDocument9 pagesHow Physical Activity Boosts Your Overall HealthankiblogsPas encore d'évaluation
- Dizziness - Vertigo and HomoeopathyDocument38 pagesDizziness - Vertigo and HomoeopathyDr. Rajneesh Kumar Sharma MD HomPas encore d'évaluation
- Circuit Weight Training in Cardiac PatientsDocument5 pagesCircuit Weight Training in Cardiac PatientsVivin YulvinaPas encore d'évaluation
- Muscle Skeletal Trauma For EMSDocument79 pagesMuscle Skeletal Trauma For EMSPaulhotvw67100% (4)
- General Comparison of Health Claims With Regards To Food and Supplement Legislation in Europe, US, and CanadaDocument4 pagesGeneral Comparison of Health Claims With Regards To Food and Supplement Legislation in Europe, US, and CanadaBudi Utami WibawaniPas encore d'évaluation