Vous aimerez peut-être aussi
- Transfusion Medicine and Hemostasis: Clinical and Laboratory AspectsD'EverandTransfusion Medicine and Hemostasis: Clinical and Laboratory AspectsÉvaluation : 4 sur 5 étoiles4/5 (9)
- Anemia-2: Overview and Select Cases: Marc Zumberg Associate Professor Division of Hematology/OncologyDocument95 pagesAnemia-2: Overview and Select Cases: Marc Zumberg Associate Professor Division of Hematology/OncologyDenise CssPas encore d'évaluation
- Anemia 101-Case StudiesDocument20 pagesAnemia 101-Case StudiesZamharira MuslimPas encore d'évaluation
- Hematology CasesDocument27 pagesHematology Casessamkad214100% (2)
- Approach To Hemolytic AnemiasDocument41 pagesApproach To Hemolytic AnemiasAmit KinarePas encore d'évaluation
- Anemia CasesDocument35 pagesAnemia CasesBogdan UrichianuPas encore d'évaluation
- Handout 2 1522436248 PDFDocument82 pagesHandout 2 1522436248 PDFHarnadi WonogiriPas encore d'évaluation
- Case Studies HemaDocument6 pagesCase Studies HemaJuan Andre' MarquinezPas encore d'évaluation
- Static OmarDocument61 pagesStatic OmarDh CndnPas encore d'évaluation
- 9a. Red Cell DisordersDocument46 pages9a. Red Cell DisordersMuhammad DaviqPas encore d'évaluation
- RBC DisordersDocument49 pagesRBC DisordersGeraldine AgpesPas encore d'évaluation
- Thrombocytopenia Sarah WalterDocument49 pagesThrombocytopenia Sarah WalterSupicha VichaiditPas encore d'évaluation
- Null 1Document49 pagesNull 1ImamAbdyPas encore d'évaluation
- ICU Blood Transfusion & Electrolytes DisturbanceDocument26 pagesICU Blood Transfusion & Electrolytes Disturbancef6080683Pas encore d'évaluation
- Abnormal CBC - PresentationDocument23 pagesAbnormal CBC - PresentationMateen ShukriPas encore d'évaluation
- Aplastic Anaemia: DR Sandeep M R Physician Jayanagar General Hospial BangaloreDocument26 pagesAplastic Anaemia: DR Sandeep M R Physician Jayanagar General Hospial BangaloreSandeep m rPas encore d'évaluation
- OncologyDocument31 pagesOncologyapi-195799092Pas encore d'évaluation
- Issues in The Diagnosis and Management of Thombocytopenic DisordersDocument45 pagesIssues in The Diagnosis and Management of Thombocytopenic Disorderspeter_mrPas encore d'évaluation
- HemaDocument59 pagesHemaSteph VeePas encore d'évaluation
- New Psychiatry FAE2016Document120 pagesNew Psychiatry FAE2016omarPas encore d'évaluation
- Anemia HemolitikDocument83 pagesAnemia HemolitikWinda A. PanjaitanPas encore d'évaluation
- Transfusion Medicine by Dr. Sharad JohriDocument54 pagesTransfusion Medicine by Dr. Sharad JohriShashwat JohriPas encore d'évaluation
- Red Cell DisordersDocument46 pagesRed Cell DisordersSofi Nur FitriaPas encore d'évaluation
- Severe Thrombocytopenia Secondary To Alcohol Use Article JournalDocument3 pagesSevere Thrombocytopenia Secondary To Alcohol Use Article JournalAulia ZrPas encore d'évaluation
- Peripheral Smear: Daniel McfarlandDocument31 pagesPeripheral Smear: Daniel McfarlandDaniel McFarlandPas encore d'évaluation
- Approach To Anemia: Bisrat DDocument45 pagesApproach To Anemia: Bisrat Dyared getachewPas encore d'évaluation
- Anemia: Case PresentationDocument7 pagesAnemia: Case PresentationNoorikiran HarisPas encore d'évaluation
- Various TopicsDocument8 pagesVarious TopicsLindsay WeissPas encore d'évaluation
- Mod9Week2 - PA 3306 - Aug 28& Sept1Document46 pagesMod9Week2 - PA 3306 - Aug 28& Sept1komal sheikhPas encore d'évaluation
- Blood and Its ComponentsDocument30 pagesBlood and Its ComponentskushalPas encore d'évaluation
- Topic 2. CBC Part 1 2021-02-26 at 11.03.32 PMDocument113 pagesTopic 2. CBC Part 1 2021-02-26 at 11.03.32 PMSub 7 Grp 3Pas encore d'évaluation
- Haematology- أسرة العطاءDocument20 pagesHaematology- أسرة العطاءThana AlameenPas encore d'évaluation
- An Approach To Anemia 4-3-03: - Bob Richard - Faculty - Washington.edu/rrichard Connect To Talks For HandoutDocument77 pagesAn Approach To Anemia 4-3-03: - Bob Richard - Faculty - Washington.edu/rrichard Connect To Talks For HandoutYen-Jen SungPas encore d'évaluation
- Abnormal Clinical Chemistry & TDM in CancerDocument44 pagesAbnormal Clinical Chemistry & TDM in CancerkinjalkaPas encore d'évaluation
- CBC GuidelineDocument95 pagesCBC GuidelineYoung MilkPas encore d'évaluation
- Journal Reading - INTERNADocument33 pagesJournal Reading - INTERNAVELISITAS ANA MARIA POTESPas encore d'évaluation
- Leukamia and Transfusion MedicineDocument26 pagesLeukamia and Transfusion MedicineSamuel kuriaPas encore d'évaluation
- Case Study - Group 5-Sem 4Document36 pagesCase Study - Group 5-Sem 4Ah BoonPas encore d'évaluation
- Heamatological Disorder: Disorder Related To Red Blood CellDocument12 pagesHeamatological Disorder: Disorder Related To Red Blood CellHelmiPas encore d'évaluation
- Medical Management of Anaemia & Case StudiesDocument39 pagesMedical Management of Anaemia & Case Studiessamrawitmekonnen16Pas encore d'évaluation
- Final Flags WorkshopDocument29 pagesFinal Flags WorkshopcandiddreamsPas encore d'évaluation
- Thalassemia: Presented By: Arpita SahaDocument32 pagesThalassemia: Presented By: Arpita Sahainterna MANADO100% (1)
- Thalassemia: Presented By: Arpita SahaDocument32 pagesThalassemia: Presented By: Arpita Sahainterna MANADOPas encore d'évaluation
- Case StudiesDocument59 pagesCase Studiesstivana26100% (1)
- Case Study Anemia-1Document6 pagesCase Study Anemia-1Melsya H UtamiPas encore d'évaluation
- Blood ProductsDocument70 pagesBlood Productsjadhamade339Pas encore d'évaluation
- OSCE HeamatologyDocument32 pagesOSCE HeamatologybnivePas encore d'évaluation
- Blood Transfusion Basic Concepts Blood Transfusion inDocument103 pagesBlood Transfusion Basic Concepts Blood Transfusion iniahmad9Pas encore d'évaluation
- Transfusion Medicine: DR Abdullah AnsariDocument53 pagesTransfusion Medicine: DR Abdullah AnsariFabsPas encore d'évaluation
- Cancer and The KidneyDocument29 pagesCancer and The Kidney[ qιlα ]Pas encore d'évaluation
- Medical Surgical Nursing - NeuroDocument19 pagesMedical Surgical Nursing - NeuroChristian EstevesPas encore d'évaluation
- CBC Interpetation Dr. MuslehDocument37 pagesCBC Interpetation Dr. MuslehMusleh Al MusalhiPas encore d'évaluation
- Haematology Sample MCQ and Emq QuestionsDocument3 pagesHaematology Sample MCQ and Emq QuestionsDr-Sumanta BanerjeePas encore d'évaluation
- Anemia Workshop1Document80 pagesAnemia Workshop1api-3762917Pas encore d'évaluation
- ProstateDocument7 pagesProstateGabriela ValdiviaPas encore d'évaluation
- Adrenal CrisisDocument27 pagesAdrenal CrisissayednourPas encore d'évaluation
- Exam 19 BloodDocument8 pagesExam 19 BloodPurwa RanePas encore d'évaluation
- Surgery of Kidney Ureter and VaricoseDocument55 pagesSurgery of Kidney Ureter and VaricoseSaurabh SharmaPas encore d'évaluation
- PAPDI DR Mardiah Suci Hardianti - Case Study ThrombocytopeniaDocument43 pagesPAPDI DR Mardiah Suci Hardianti - Case Study ThrombocytopeniaMarcelliaPas encore d'évaluation
- Wln-Normal LabourDocument45 pagesWln-Normal LabourEmmanuel MukukaPas encore d'évaluation
- Obgy-Wln Late Pregnancy Complications: Kabwe Central HospitalDocument15 pagesObgy-Wln Late Pregnancy Complications: Kabwe Central HospitalEmmanuel MukukaPas encore d'évaluation
- Neonatal Sepsis (NNS) : DR Jerome SiyambuDocument37 pagesNeonatal Sepsis (NNS) : DR Jerome SiyambuEmmanuel MukukaPas encore d'évaluation
- Hydro Cep Hal UsDocument11 pagesHydro Cep Hal UsEmmanuel MukukaPas encore d'évaluation
- Seizure Disorders: Musupila.M DCM, Adgm, BSC Cs (Unza) 6 November 2019Document26 pagesSeizure Disorders: Musupila.M DCM, Adgm, BSC Cs (Unza) 6 November 2019Emmanuel MukukaPas encore d'évaluation
- Peptic Ulcers: DR Yotham Phiri Mmed (Surg)Document46 pagesPeptic Ulcers: DR Yotham Phiri Mmed (Surg)Emmanuel MukukaPas encore d'évaluation
- Kabwe Central Hospital KCH: Breast Cancer"Document34 pagesKabwe Central Hospital KCH: Breast Cancer"Emmanuel MukukaPas encore d'évaluation
- Cerebral Palsy 08.04.15 LectureDocument25 pagesCerebral Palsy 08.04.15 LectureEmmanuel MukukaPas encore d'évaluation
- Kabwe Central Hospital: "Hydrocephalus"Document39 pagesKabwe Central Hospital: "Hydrocephalus"Emmanuel MukukaPas encore d'évaluation
- Kabwe Central Hospital Surgery: Wisdom's Lecture NotesDocument24 pagesKabwe Central Hospital Surgery: Wisdom's Lecture NotesEmmanuel MukukaPas encore d'évaluation
- Flu Vaccine: Information For People at RiskDocument8 pagesFlu Vaccine: Information For People at Riskkovi mPas encore d'évaluation
- CTG Interpretation of CTG and CFHM During Antepartum and Intrapartum Periods Ho Lai FongDocument33 pagesCTG Interpretation of CTG and CFHM During Antepartum and Intrapartum Periods Ho Lai FongSabrina AzizPas encore d'évaluation
- Coding With ModifiersDocument144 pagesCoding With ModifiersRohan Kulkarni100% (2)
- Icpc 2 R PDFDocument204 pagesIcpc 2 R PDFagni sukma fahiraPas encore d'évaluation
- Pneumonia (Pulmonya)Document33 pagesPneumonia (Pulmonya)LopaoMedinaPas encore d'évaluation
- Adime For DiabetesDocument2 pagesAdime For Diabetesapi-383891195Pas encore d'évaluation
- Buildings and Structures: Padua EsteDocument2 pagesBuildings and Structures: Padua EsteKevin LavinaPas encore d'évaluation
- Abnormal Psychology 6th Edition Nolen-Hoeksema Solutions Manual 1Document26 pagesAbnormal Psychology 6th Edition Nolen-Hoeksema Solutions Manual 1jamie100% (31)
- Module 6 Case Study - Raul SalazarDocument2 pagesModule 6 Case Study - Raul Salazarapi-296420201Pas encore d'évaluation
- Lymph Notes E.N.T MQsDocument65 pagesLymph Notes E.N.T MQsAli QuwarahPas encore d'évaluation
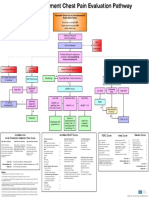
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidPas encore d'évaluation
- Similarities and Differences VocabularyDocument9 pagesSimilarities and Differences VocabularyAliPas encore d'évaluation
- Spinal Exercise Home ProgrammeDocument19 pagesSpinal Exercise Home ProgrammePrabha VetrichelvanPas encore d'évaluation
- Covid GuidelinesDocument1 pageCovid Guidelinesapi-509452068Pas encore d'évaluation
- Goddess Isis - 7D InitiationDocument6 pagesGoddess Isis - 7D InitiationEmeraldRayPas encore d'évaluation
- Cuddon - Electrophysiology in Neuromuscular Disease - 2002Document32 pagesCuddon - Electrophysiology in Neuromuscular Disease - 2002paula gonzalezPas encore d'évaluation
- INTRODUCTION A Toddler Is A Young ChildDocument13 pagesINTRODUCTION A Toddler Is A Young Childlovely_epsPas encore d'évaluation
- Communicable Disease Epidemiology: "Anthrax"Document9 pagesCommunicable Disease Epidemiology: "Anthrax"Eko PurwatiPas encore d'évaluation
- Orbit (Kankis)Document42 pagesOrbit (Kankis)Jel JelitaaaPas encore d'évaluation
- Funk Roberts Spartan Training System 4 Week Workout ChallengeDocument25 pagesFunk Roberts Spartan Training System 4 Week Workout ChallengeValeska A. Cortés Licuime100% (1)
- NCPDocument7 pagesNCPJulianne Jeamer FabroaPas encore d'évaluation
- Mentha Cordifelia TeaDocument10 pagesMentha Cordifelia TeaMia Pearl Tabios ValenzuelaPas encore d'évaluation
- Takayasu S Arter It IsDocument5 pagesTakayasu S Arter It IsButarbutar MelvaPas encore d'évaluation
- Walter Modell M. D., F.A.C.P., Doris J. Place R. N. (Auth.) - The Use of Drugs - Principles of Pharmacology and Therapeutics For Nurses (1957, Springer-Verlag Berlin Heidelberg) PDFDocument350 pagesWalter Modell M. D., F.A.C.P., Doris J. Place R. N. (Auth.) - The Use of Drugs - Principles of Pharmacology and Therapeutics For Nurses (1957, Springer-Verlag Berlin Heidelberg) PDFbluegreenalgaPas encore d'évaluation
- Polyherbal Formulations Based On Indian Medicinal Plants As Antidiabetic PhytotherapeuticsDocument15 pagesPolyherbal Formulations Based On Indian Medicinal Plants As Antidiabetic PhytotherapeuticsJohnnPas encore d'évaluation
- Occupational Health Pre-Employment Health Assessment Form March 08Document4 pagesOccupational Health Pre-Employment Health Assessment Form March 08queenmombi100% (2)
- Activities-Specific Balance Confidence (Abc) ScaleDocument16 pagesActivities-Specific Balance Confidence (Abc) ScaleMochammad Syarif HidayatPas encore d'évaluation
- Mapeh Grade 8 Third QuarterDocument4 pagesMapeh Grade 8 Third QuarterPhilip Jansen Guarin100% (2)
- Department of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaDocument106 pagesDepartment of Family Medicine Fpe Headache Syndrome: - Vanaveera Pandian SwethaSuba Saravanan 12Pas encore d'évaluation
- Thesis English 4Document21 pagesThesis English 4Hermiie Joii Galang MaglaquiiPas encore d'évaluation