Vous aimerez peut-être aussi
- Wound Management for the Advanced PractitionerD'EverandWound Management for the Advanced PractitionerÉvaluation : 2 sur 5 étoiles2/5 (2)
- Wound Care Basics: Types, Staging, Assessment & TreatmentDocument26 pagesWound Care Basics: Types, Staging, Assessment & TreatmentIntan Purnamasari100% (1)
- Wound Case Study AssessmentDocument7 pagesWound Case Study Assessmentcass1526100% (2)
- Wound Dressing GuideDocument2 pagesWound Dressing Guidekitsil100% (6)
- Clinical Applied Anatomy in Wound CareDocument18 pagesClinical Applied Anatomy in Wound CareKlinik Komuniti Perwira100% (2)
- Wound Care PDFDocument100 pagesWound Care PDFVanessaMUeller100% (2)
- Wound Care ModuleDocument29 pagesWound Care ModuleCaleb Fellowes100% (1)
- Wound Care Selection Guide (2011)Document2 pagesWound Care Selection Guide (2011)iliePas encore d'évaluation
- Wound Dressing Guide PDFDocument2 pagesWound Dressing Guide PDFrufftuffcookiePas encore d'évaluation
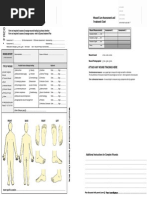
- Attach Any Wound Tracings Here Attach Any Wound Tracings HereDocument2 pagesAttach Any Wound Tracings Here Attach Any Wound Tracings Herewiwi handayani100% (1)
- Wound CareDocument617 pagesWound CareBakti SetiawanPas encore d'évaluation
- Wound Care Manual, Malaysia MOHDocument199 pagesWound Care Manual, Malaysia MOHmfuadj92% (13)
- Wound Care Products: Department of Podiatric SurgeryDocument44 pagesWound Care Products: Department of Podiatric Surgerydrkbarry100% (6)
- Wound ManagementDocument86 pagesWound ManagementRăzvanAndrei67% (3)
- Suturing WorkshopDocument87 pagesSuturing WorkshopVictor OpreaPas encore d'évaluation
- Wound Healing and Wound CareDocument7 pagesWound Healing and Wound CareCarl Earvin L. FavoritoPas encore d'évaluation
- 3 Wound CareDocument14 pages3 Wound Caresechzhen83% (6)
- 50 IV Therapy Tips and TricksDocument10 pages50 IV Therapy Tips and TricksAmar Freebiker Abaza0% (1)
- 409 Pope, B. and Maillie, S. CCRN-PCCN Review Multisystem and Q and ADocument21 pages409 Pope, B. and Maillie, S. CCRN-PCCN Review Multisystem and Q and Agliftan100% (2)
- Wound Care: Jocelyn M. Lledo, MDDocument67 pagesWound Care: Jocelyn M. Lledo, MDJaslin HerbsPas encore d'évaluation
- OPQRSTDocument2 pagesOPQRSTHarsah BahtiarPas encore d'évaluation
- Wound ClassificationDocument48 pagesWound Classificationzarizi100% (2)
- Wounds and Wound CareDocument26 pagesWounds and Wound Careapi-3697326100% (1)
- Wound CareDocument11 pagesWound Carenichole9981Pas encore d'évaluation
- Wound Care GuideDocument36 pagesWound Care GuideDivina D Galvez-BeronioPas encore d'évaluation
- Pope, B. CCRN-PCCN-CMC Review Endocrine and BehavioralDocument14 pagesPope, B. CCRN-PCCN-CMC Review Endocrine and BehavioralKeisha JenkinsPas encore d'évaluation
- Standards For Wound Prevention and Management 2016Document66 pagesStandards For Wound Prevention and Management 2016sidney drecottePas encore d'évaluation
- 12 Lead ECG Mod 1Document31 pages12 Lead ECG Mod 1johnmmenahPas encore d'évaluation
- 2.1. Pre-Operative NursingDocument130 pages2.1. Pre-Operative Nursingnoo.wannPas encore d'évaluation
- Wound ManagementDocument72 pagesWound Managementdrsonuchawla100% (1)
- Sutures and Suturing: Dr. Sameer A. MokeemDocument63 pagesSutures and Suturing: Dr. Sameer A. Mokeemwindshock100% (1)
- Icu NotesDocument47 pagesIcu NotesChryst Louise SaavedraPas encore d'évaluation
- Inflammation and Wound HealingDocument3 pagesInflammation and Wound HealingPrincess AgarwalPas encore d'évaluation
- PDF - VeinsDocument3 pagesPDF - VeinsjulialeoPas encore d'évaluation
- Chapter 4 CNADocument34 pagesChapter 4 CNALisa Williams-WashingtonPas encore d'évaluation
- Skin Integrity and Wound CareDocument84 pagesSkin Integrity and Wound CareerninurhayatiPas encore d'évaluation
- Wound CareDocument10 pagesWound CareKenima Idao100% (3)
- Perioperative NursingDocument253 pagesPerioperative NursingCherr May Olesco - Nalasa100% (4)
- Critical Care Note PDFDocument10 pagesCritical Care Note PDFlml100% (1)
- Orthopedic NursingDocument150 pagesOrthopedic NursingCyrhille Paner100% (1)
- Texbook of Emergency CardiologyDocument445 pagesTexbook of Emergency CardiologyArtur TarsaPas encore d'évaluation
- Family Nursing Process GuideDocument77 pagesFamily Nursing Process GuideEmmanuelPas encore d'évaluation
- Trauma NursingDocument35 pagesTrauma NursingGodwin Babista Gonzales100% (2)
- Perioperative Nursing Core ConceptsDocument67 pagesPerioperative Nursing Core ConceptsYucef Bahian-AbangPas encore d'évaluation
- Wound Care GuideDocument30 pagesWound Care Guiderumaisha100% (2)
- Basic Suturing Skills Booklet+Document34 pagesBasic Suturing Skills Booklet+Rohit Agrawal100% (3)
- ~Document832 pages~Afra Hanifi100% (1)
- CL-078 Wound Assessment Guideline 2015Document35 pagesCL-078 Wound Assessment Guideline 2015JovialPas encore d'évaluation
- CCRN-PCCN Review GastrointestinalDocument23 pagesCCRN-PCCN Review GastrointestinalGiovanni MictilPas encore d'évaluation
- Fundamental of NursingDocument993 pagesFundamental of NursingSyed BuRhan Ud-Din100% (3)
- History of The Suture Personal Suture Preference Suture CharacteristicsDocument33 pagesHistory of The Suture Personal Suture Preference Suture Characteristicsmob3Pas encore d'évaluation
- Wound Assessment and DocumentationDocument66 pagesWound Assessment and DocumentationRiaReimannPas encore d'évaluation
- Notes For Perioperative NursingDocument5 pagesNotes For Perioperative NursingNey JunePas encore d'évaluation
- Med MathDocument22 pagesMed Mathmeanne073Pas encore d'évaluation
- Common Skin Conditions in Wound CareDocument8 pagesCommon Skin Conditions in Wound Carelina febriantiPas encore d'évaluation
- Preskas Bedah Plastik NeonizaDocument30 pagesPreskas Bedah Plastik NeonizaRaPas encore d'évaluation
- Examination of Head and Neck SwellingsDocument22 pagesExamination of Head and Neck SwellingsObehi EromoselePas encore d'évaluation
- Cutaneous Ulcers HFHDocument52 pagesCutaneous Ulcers HFHEmmanuel Papa AcquahPas encore d'évaluation
- Oeste o ArthritisDocument29 pagesOeste o ArthritisElamathi PhysioPas encore d'évaluation
- Why Wounds Fail To HealDocument6 pagesWhy Wounds Fail To HealMsPocketbook HoarderPas encore d'évaluation
- Physical ExaminationDocument117 pagesPhysical ExaminationJan Oliver YaresPas encore d'évaluation
- Issue 23Document2 pagesIssue 23ppni lembataPas encore d'évaluation
- Pain Assess in Older Adults PDFDocument2 pagesPain Assess in Older Adults PDFJan Oliver YaresPas encore d'évaluation
- Principles of Palliative CareDocument12 pagesPrinciples of Palliative CareJan Oliver YaresPas encore d'évaluation
- Pain Assess in Older Adults PDFDocument2 pagesPain Assess in Older Adults PDFJan Oliver YaresPas encore d'évaluation
- NCM 107n/L Care of Mother, Child and Adolescent (Well ClientDocument37 pagesNCM 107n/L Care of Mother, Child and Adolescent (Well ClientJan Oliver YaresPas encore d'évaluation
- NCM 107n/L Care of Mother, Child and Adolescent (Well ClientDocument37 pagesNCM 107n/L Care of Mother, Child and Adolescent (Well ClientJan Oliver YaresPas encore d'évaluation
- Unang Yakap: Essential Newborn Care (ENC) ProtocolDocument13 pagesUnang Yakap: Essential Newborn Care (ENC) ProtocolJan Oliver YaresPas encore d'évaluation
- Postpartum CareDocument56 pagesPostpartum CareJan Oliver YaresPas encore d'évaluation
- Meds Affecting ReproDocument52 pagesMeds Affecting ReproJan Oliver YaresPas encore d'évaluation
- Geriatric AssessmentDocument63 pagesGeriatric AssessmentJan Oliver Yares100% (1)
- Framework For MCNDocument50 pagesFramework For MCNJan Oliver YaresPas encore d'évaluation
- Framework For MCHDocument7 pagesFramework For MCHJan Oliver YaresPas encore d'évaluation
- Evidence-Based Practice in Maternal & Child HealthDocument15 pagesEvidence-Based Practice in Maternal & Child HealthJan Oliver YaresPas encore d'évaluation
- Postpartum CareDocument56 pagesPostpartum CareJan Oliver YaresPas encore d'évaluation
- Framework For MCHDocument7 pagesFramework For MCHJan Oliver YaresPas encore d'évaluation
- NCM 107n/L Care of Mother, Child and Adolescent (Well ClientDocument37 pagesNCM 107n/L Care of Mother, Child and Adolescent (Well ClientJan Oliver YaresPas encore d'évaluation
- Rozzano Locsin's Technological Caring Model of NursingDocument22 pagesRozzano Locsin's Technological Caring Model of NursingJan Oliver YaresPas encore d'évaluation
- Intrapartal - Theories of LaborDocument21 pagesIntrapartal - Theories of LaborJan Oliver YaresPas encore d'évaluation
- Fulmer Spices: Comprehensive Assessment Tool For Older AdultsDocument9 pagesFulmer Spices: Comprehensive Assessment Tool For Older AdultsJan Oliver YaresPas encore d'évaluation
- Nursing Standard of Practice Protocol: Iatrogenesis: The Nurse's Role in Preventing Patient HarmDocument14 pagesNursing Standard of Practice Protocol: Iatrogenesis: The Nurse's Role in Preventing Patient HarmJan Oliver YaresPas encore d'évaluation
- Activity 2Document5 pagesActivity 2Jan Oliver YaresPas encore d'évaluation
- Ida Jean OrlandoDocument13 pagesIda Jean OrlandoJan Oliver Yares100% (1)
- Drugs For Repro System-1Document67 pagesDrugs For Repro System-1Jan Oliver YaresPas encore d'évaluation
- Theories Relevant To Nursing Practice: Gladys C. Yares, RN RMDocument75 pagesTheories Relevant To Nursing Practice: Gladys C. Yares, RN RMJan Oliver YaresPas encore d'évaluation
- 106n CONCEPTUAL MODELSDocument25 pages106n CONCEPTUAL MODELSJan Oliver YaresPas encore d'évaluation
- Developmental TheoryDocument27 pagesDevelopmental TheoryJan Oliver YaresPas encore d'évaluation
- Organ DonationDocument31 pagesOrgan DonationJan Oliver Yares100% (1)
- Bioethicshxcare Issues TopicsDocument22 pagesBioethicshxcare Issues TopicsJan Oliver Yares100% (1)
- Theories and Principles of Health EthicsDocument18 pagesTheories and Principles of Health EthicsJan Oliver YaresPas encore d'évaluation
- AFFERENT & EFFERENT SyndromeDocument12 pagesAFFERENT & EFFERENT SyndromeAli Sibra MulluziPas encore d'évaluation
- Lumbar PunctureDocument23 pagesLumbar Puncturemamoon100% (2)
- Hydraulic Fracture Mechanics: Peter Valk6 Michael EconomidesDocument6 pagesHydraulic Fracture Mechanics: Peter Valk6 Michael EconomidesAdib Wahyu HidayatPas encore d'évaluation
- Ergo 4 WeldersDocument32 pagesErgo 4 WeldersjoessterPas encore d'évaluation
- Acute Anterior Cruciate Ligament Rupture: Repair or Reconstruction?Document11 pagesAcute Anterior Cruciate Ligament Rupture: Repair or Reconstruction?Mohan DesaiPas encore d'évaluation
- Chapter 16 ITLS - 04-2020Document20 pagesChapter 16 ITLS - 04-2020Ahyar MohPas encore d'évaluation
- Dressings: Carmina Disu Diana Ray Margarita DialaDocument15 pagesDressings: Carmina Disu Diana Ray Margarita DialaNdor BariboloPas encore d'évaluation
- Wildlings JDRDocument8 pagesWildlings JDRRodrigo PenaPas encore d'évaluation
- Stone Dwarf, Stone Sorcerer and Warlock Patron of The DaoDocument11 pagesStone Dwarf, Stone Sorcerer and Warlock Patron of The DaoRonHoward100% (1)
- The Vanishing Throne: Book Two of The Falconer Trilogy (Excerpt)Document24 pagesThe Vanishing Throne: Book Two of The Falconer Trilogy (Excerpt)ChronicleBooks0% (1)
- Ortho McqsDocument3 pagesOrtho McqsMohamed Shafi67% (3)
- DLP Domestic ViolenceDocument2 pagesDLP Domestic ViolenceRosel LibradoPas encore d'évaluation
- Wound Types and Treatment GuideDocument4 pagesWound Types and Treatment GuideNikki Ann Kanapi FernandezPas encore d'évaluation
- Download Sustain A Workplace Rockstar Romance Rhapsody Series 5 Amy Booker full chapterDocument67 pagesDownload Sustain A Workplace Rockstar Romance Rhapsody Series 5 Amy Booker full chaptermelissa.maglori550100% (5)
- YOGA Guidebook 7 Simple Yoga Poses You Should Try YOGA Guidebook (AUSTIN, THOMPSON) (Z-Library)Document35 pagesYOGA Guidebook 7 Simple Yoga Poses You Should Try YOGA Guidebook (AUSTIN, THOMPSON) (Z-Library)amitlkoyogaPas encore d'évaluation
- Commercial Jet Accidents Report 1959-2005Document26 pagesCommercial Jet Accidents Report 1959-2005nerminaPas encore d'évaluation
- Knee InjuryDocument44 pagesKnee Injuryhendi_filipus_90Pas encore d'évaluation
- Case Study 7 8 and 9Document32 pagesCase Study 7 8 and 9Lyca Ledesma JamonPas encore d'évaluation
- Skaven Magic ItemDocument2 pagesSkaven Magic ItemBasterd Merchant100% (1)
- Assessing PainDocument2 pagesAssessing Painindri yaniPas encore d'évaluation
- Toolbox Talk 4 Manual HandlingDocument2 pagesToolbox Talk 4 Manual HandlingSajid HussainPas encore d'évaluation
- Questions To Ask When Answering OMFS BleepDocument4 pagesQuestions To Ask When Answering OMFS BleepNeelam Rathod MehtaPas encore d'évaluation
- Back Injuries in ConstructionDocument3 pagesBack Injuries in ConstructionNurPas encore d'évaluation
- Revised Holistic Care PlanDocument5 pagesRevised Holistic Care Planapi-357119001Pas encore d'évaluation
- Original PDF Human Anatomy 5th Edition by Michael Mckinley PDFDocument41 pagesOriginal PDF Human Anatomy 5th Edition by Michael Mckinley PDFjames.auiles49297% (34)
- Foreign-Body Airway ObstructionDocument17 pagesForeign-Body Airway ObstructionDessy Christiani Part IIPas encore d'évaluation
- Acutepain PneumoniaDocument3 pagesAcutepain PneumoniaJoy SalvadorPas encore d'évaluation
- Richie Brace Treating DropfootDocument2 pagesRichie Brace Treating Dropfootakhmad ulilPas encore d'évaluation
- SMM3Document194 pagesSMM3shagggadellicPas encore d'évaluation
- Karakter 108 SOD Suikoden 2Document87 pagesKarakter 108 SOD Suikoden 2Vatjarr IlNuovoPas encore d'évaluation