Vous aimerez peut-être aussi
- Primitive Man and His Food - Arnold DeVriesDocument97 pagesPrimitive Man and His Food - Arnold DeVriessamui11Pas encore d'évaluation
- Placenta Previa and Abruptio Placenta: Presenter Eessaa ShresthaDocument72 pagesPlacenta Previa and Abruptio Placenta: Presenter Eessaa ShresthaEsa SthaPas encore d'évaluation
- Prenatal Brochure 2011-FF - Health Power For MinoritiesDocument2 pagesPrenatal Brochure 2011-FF - Health Power For MinoritiesNorma J. Goodwin, MDPas encore d'évaluation
- User Manual For Applications Xformer Exe EnglishLightDocument51 pagesUser Manual For Applications Xformer Exe EnglishLightNunoClaudinoPas encore d'évaluation
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Preparing A Family For Childbirth and ParentingDocument5 pagesPreparing A Family For Childbirth and ParentingBern NerquitPas encore d'évaluation
- PostpartumDocument3 pagesPostpartumMuhammad RifaiPas encore d'évaluation
- Normal Labor and DeliveryDocument8 pagesNormal Labor and DeliveryMark Joshua CervantesPas encore d'évaluation
- Nursing Management TrueDocument46 pagesNursing Management TrueTriplet 727 Triplet 727Pas encore d'évaluation
- PostpartumDischarge PDFDocument6 pagesPostpartumDischarge PDFhudaPas encore d'évaluation
- Tocolytic Treatment in PregnancyDocument21 pagesTocolytic Treatment in PregnancyxxdrivexxPas encore d'évaluation
- Maternal and Child HealthDocument7 pagesMaternal and Child HealthNessa Layos MorilloPas encore d'évaluation
- Bachelor of Science in Nursing: Francar Jade M. de Vera BSN - N16Document10 pagesBachelor of Science in Nursing: Francar Jade M. de Vera BSN - N16Francar Jade De Vera100% (1)
- Case PresDocument100 pagesCase PresJoj BagnatePas encore d'évaluation
- 8. Care of Child With GI Dysfunction (1) ءءءءDocument44 pages8. Care of Child With GI Dysfunction (1) ءءءءNuhaPas encore d'évaluation
- OB Case StudyDocument20 pagesOB Case Studylms93093Pas encore d'évaluation
- Alternative Methods of BirthDocument8 pagesAlternative Methods of BirthDn CrediblePas encore d'évaluation
- 2-Checklist For Pelvis AssessmentDocument3 pages2-Checklist For Pelvis AssessmentGazala ParveenPas encore d'évaluation
- Breast FeedingDocument11 pagesBreast FeedingJoana Marie GuanPas encore d'évaluation
- Updated Universal Precautions Guideline GGRDocument3 pagesUpdated Universal Precautions Guideline GGRapi-501821819Pas encore d'évaluation
- Newborn Screening Policy Catarman Doctors Hospital, Inc.: University of Eastern PhilippinesDocument7 pagesNewborn Screening Policy Catarman Doctors Hospital, Inc.: University of Eastern PhilippinesGenn Medrano GirayPas encore d'évaluation
- DOH Programs EEINC Newborn Screening BEmONC CEmONC NutritionDocument46 pagesDOH Programs EEINC Newborn Screening BEmONC CEmONC NutritionKRISTINE ANGELIE PANESPas encore d'évaluation
- Clinical Week 3 - Teaching Plan - BreastfeedingDocument2 pagesClinical Week 3 - Teaching Plan - Breastfeedingapi-273168705Pas encore d'évaluation
- Rubella and PregnancyDocument6 pagesRubella and PregnancyKABERA RENEPas encore d'évaluation
- DispencingDocument19 pagesDispencingushaeatakotaPas encore d'évaluation
- AH1N1 PPT PresentationDocument28 pagesAH1N1 PPT PresentationIna Isabela CostiboloPas encore d'évaluation
- 4 Pain Management, Theories of Labor Onset, Signs of LaborDocument31 pages4 Pain Management, Theories of Labor Onset, Signs of Labormamsh KlangPas encore d'évaluation
- Letter of ApplicationDocument4 pagesLetter of Applicationmelai_0123Pas encore d'évaluation
- FAMILY PLANNING PROGRAM HandoutsDocument2 pagesFAMILY PLANNING PROGRAM HandoutsWilma Nierva BeraldePas encore d'évaluation
- GDM TeachingprojectDocument2 pagesGDM Teachingprojectapi-285033848Pas encore d'évaluation
- A Review On Otitis Media (Karnapaka) : Ayurvedic Aspects and TreatmentDocument4 pagesA Review On Otitis Media (Karnapaka) : Ayurvedic Aspects and TreatmentEditor_IAIMPas encore d'évaluation
- Dra Juson Labor & DeliveryDocument153 pagesDra Juson Labor & DeliveryaringkinkingPas encore d'évaluation
- Discharge PlanningDocument2 pagesDischarge PlanningAthena Irish LastimosaPas encore d'évaluation
- NCM107 - Chapter 04-Lesson 3 Postpartal CareDocument22 pagesNCM107 - Chapter 04-Lesson 3 Postpartal CareJosephine LoriaPas encore d'évaluation
- Module 4 - Postpartum CareDocument5 pagesModule 4 - Postpartum CareKatie HolmesPas encore d'évaluation
- Nur 1210 Maternal Module #3 Nursing Care of The Pregnant Client (Medical)Document40 pagesNur 1210 Maternal Module #3 Nursing Care of The Pregnant Client (Medical)Allyza EspirituPas encore d'évaluation
- Newborn ScreeningDocument20 pagesNewborn Screeningfeva55Pas encore d'évaluation
- Live Preterm Baby Delivered NSDDocument13 pagesLive Preterm Baby Delivered NSDKristine Anne SorianoPas encore d'évaluation
- P-132 Leopolds-ManeuverDocument5 pagesP-132 Leopolds-ManeuverAubrey AndresPas encore d'évaluation
- Knowledge and Practice of Postnatal Mothers Regarding Personal Hygiene and Newborn CareDocument6 pagesKnowledge and Practice of Postnatal Mothers Regarding Personal Hygiene and Newborn CareUlin Nuha JazminPas encore d'évaluation
- 68 Abnormal PeuperiumDocument44 pages68 Abnormal PeuperiumGodsonYeboah-AwudziPas encore d'évaluation
- The Care of A Woman During The Third and Fourth Stages of LaborDocument16 pagesThe Care of A Woman During The Third and Fourth Stages of LaborDimple AnticamaraPas encore d'évaluation
- Method of ChildbirthDocument5 pagesMethod of ChildbirthRosmania RimaPas encore d'évaluation
- 6 Antepartum Care PDFDocument24 pages6 Antepartum Care PDFmohammed farajiPas encore d'évaluation
- Labor and Birth HandoutDocument9 pagesLabor and Birth Handoutapi-240665032Pas encore d'évaluation
- Breastfeeding Assessment Tool: Neonatal: © Unicef UK Baby Friendly Initiative, Adapted From NHS Greater Glasgow & ClydeDocument2 pagesBreastfeeding Assessment Tool: Neonatal: © Unicef UK Baby Friendly Initiative, Adapted From NHS Greater Glasgow & ClydedeboraPas encore d'évaluation
- Improve Maternal NutritionDocument14 pagesImprove Maternal NutritionRAHMI AYUDAPas encore d'évaluation
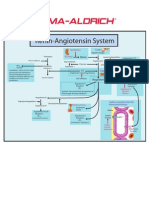
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Nursing Care of A Newborn and Family in The Post Partal Period ReviewerDocument2 pagesNursing Care of A Newborn and Family in The Post Partal Period ReviewerJo PigarPas encore d'évaluation
- Module 6 IntrapartumDocument33 pagesModule 6 IntrapartumTiangco Fatima AlfaPas encore d'évaluation
- Placenta PreviaDocument33 pagesPlacenta PreviamidoPas encore d'évaluation
- Hypertensive Disorders of Pregnancy: Mohammad Khalandar (116) Megha DDocument22 pagesHypertensive Disorders of Pregnancy: Mohammad Khalandar (116) Megha DMegha D100% (1)
- Growth and Development of Newborn To InfancyDocument54 pagesGrowth and Development of Newborn To Infancymerin sunilPas encore d'évaluation
- Health EducationDocument26 pagesHealth EducationALYSSA NICOLE GINESPas encore d'évaluation
- Percutaneous Endoscopic Gastroscopy (Peg) : Indications For Peg InsertionDocument3 pagesPercutaneous Endoscopic Gastroscopy (Peg) : Indications For Peg InsertionRicher John PolicarpioPas encore d'évaluation
- College of NursingDocument54 pagesCollege of NursingJan VillaminPas encore d'évaluation
- NCP Knowledge DeficitDocument2 pagesNCP Knowledge DeficitRainier IbarretaPas encore d'évaluation
- NUR 204 2019 Inserting A Nasogastric TubeDocument56 pagesNUR 204 2019 Inserting A Nasogastric TubeHanan DaghashPas encore d'évaluation
- Newborn Reflexes Checklist Check and Describe Each ResponseDocument2 pagesNewborn Reflexes Checklist Check and Describe Each ResponseAmina Sahar 08Pas encore d'évaluation
- Unit VIII PRESUMPTIVE SIGNS AND SYMPTOMS OF PREGNANCYDocument5 pagesUnit VIII PRESUMPTIVE SIGNS AND SYMPTOMS OF PREGNANCYNancy100% (1)
- Types of Drug Preparation (Credit To The Rightful Owner)Document1 pageTypes of Drug Preparation (Credit To The Rightful Owner)Keren Grace EspirituPas encore d'évaluation
- Newborn Umbilical Cord Care - An Evidence Based Quality ImprovemenDocument45 pagesNewborn Umbilical Cord Care - An Evidence Based Quality Improvemenelena ampatinPas encore d'évaluation
- Community Pharmacy Organization: Pharmaceutical Management.Document12 pagesCommunity Pharmacy Organization: Pharmaceutical Management.pawannnnPas encore d'évaluation
- Kankushta (One of The Uparasas in Rasashastra)Document13 pagesKankushta (One of The Uparasas in Rasashastra)Ayurveda PPT0% (1)
- Initial Nurse Patient InteractionDocument1 pageInitial Nurse Patient InteractionBryan Jay Carlo PañaPas encore d'évaluation
- Academic Regulation and Syllabus 2013-14Document135 pagesAcademic Regulation and Syllabus 2013-14Sagar MudgalPas encore d'évaluation
- Title: Artificial Intelligence in Healthcare An Integrated Approach To Healthcare DeliveryDocument13 pagesTitle: Artificial Intelligence in Healthcare An Integrated Approach To Healthcare DeliveryofhsaosdafsdfPas encore d'évaluation
- Grade 4 Chondromalacia Patella TreatmentDocument3 pagesGrade 4 Chondromalacia Patella TreatmentTroy0% (1)
- Aetna Insurance DecisionDocument13 pagesAetna Insurance DecisionJeffStelling1Pas encore d'évaluation
- Drug Therapy For PicuDocument32 pagesDrug Therapy For PicuNeethu Mariya MathewPas encore d'évaluation
- Life-Changed Self-Healing Series Ayurvedic Oil PullingDocument19 pagesLife-Changed Self-Healing Series Ayurvedic Oil PullingReverend Michael Zarchian Amjoy100% (2)
- Intestinal Malrotation and VolvulusDocument14 pagesIntestinal Malrotation and VolvulusSaf Tanggo Diampuan100% (1)
- Nabh Entry LevelDocument64 pagesNabh Entry LevelRenuka MuruganPas encore d'évaluation
- Nephrolithiasis PDFDocument21 pagesNephrolithiasis PDFAulia AlmaPas encore d'évaluation
- Direct Pulp Capping in Primary Molars: Report of Two CasesDocument3 pagesDirect Pulp Capping in Primary Molars: Report of Two Casesemie sitorusPas encore d'évaluation
- Romsons All ProductDocument53 pagesRomsons All ProductBoyke WinterbergPas encore d'évaluation
- Post Dam and Relief Chamber FullDocument35 pagesPost Dam and Relief Chamber FullnaomiPas encore d'évaluation
- AJODO-90 Petrovic Et Al Role of The Lateral Pterigoid Muscle and Menisco Temporomandibular...Document12 pagesAJODO-90 Petrovic Et Al Role of The Lateral Pterigoid Muscle and Menisco Temporomandibular...ortodoncia 2018Pas encore d'évaluation
- Cardiovascular PharmacologyDocument77 pagesCardiovascular PharmacologyDhruva PatelPas encore d'évaluation
- Pharmacology Fundamental ConceptsDocument84 pagesPharmacology Fundamental Conceptsteaforschool filesPas encore d'évaluation
- Research ProposalDocument25 pagesResearch ProposaladerindPas encore d'évaluation
- HospPharm 1.1 - DevHistoryDocument18 pagesHospPharm 1.1 - DevHistoryHeidi Jade Ong BalinasPas encore d'évaluation
- Guru AppointmentDocument2 pagesGuru AppointmentKirankumar MutnaliPas encore d'évaluation
- Literature Review On IbuprofenDocument8 pagesLiterature Review On Ibuprofenbujuj1tunag2100% (1)
- Vitamin A Natural SourcesDocument3 pagesVitamin A Natural Sourceszoezoe87Pas encore d'évaluation
- National Standards and Minimum Service Package For Adolescent and Youth-Friendly Health Services in NigeriaDocument90 pagesNational Standards and Minimum Service Package For Adolescent and Youth-Friendly Health Services in NigeriaDMDGPas encore d'évaluation
- September 2013 Exam QuestionsDocument13 pagesSeptember 2013 Exam QuestionsooiziungiePas encore d'évaluation
- Biology Investigatory Project: TopicDocument13 pagesBiology Investigatory Project: TopicRaj SahuPas encore d'évaluation
- Eccrine Sweat GlandsDocument5 pagesEccrine Sweat GlandssakuraleeshaoranPas encore d'évaluation