Vous aimerez peut-être aussi
- Vier Marleiny, Melena Gastropathy Nsaid, Duty HannaDocument19 pagesVier Marleiny, Melena Gastropathy Nsaid, Duty HannaHanna GustinPas encore d'évaluation
- Yuniarti, CHF, Krisis Tiroid, CAP Duty HannaDocument17 pagesYuniarti, CHF, Krisis Tiroid, CAP Duty HannaHanna GustinPas encore d'évaluation
- Yusnimar, Penkes Ec SAE, Duty HannaDocument18 pagesYusnimar, Penkes Ec SAE, Duty HannaHanna GustinPas encore d'évaluation
- Yetti, CAP Hipoxia, Duty HannaDocument18 pagesYetti, CAP Hipoxia, Duty HannaHanna GustinPas encore d'évaluation
- Yulnova, Acute On CKD and Thrombocytopenia, Duty HannaDocument18 pagesYulnova, Acute On CKD and Thrombocytopenia, Duty HannaHanna GustinPas encore d'évaluation
- Neli Pastinar, Penkes UE, RPGN, SLE, Duty HannaDocument19 pagesNeli Pastinar, Penkes UE, RPGN, SLE, Duty HannaHanna GustinPas encore d'évaluation
- Nilawati. GEA With Severe Dehydration, Duty HannaDocument19 pagesNilawati. GEA With Severe Dehydration, Duty HannaHanna GustinPas encore d'évaluation
- Heri Sunoto, CKD CHF, Duty HannaDocument17 pagesHeri Sunoto, CKD CHF, Duty HannaHanna GustinPas encore d'évaluation
- Muhammad Nur, Penkes Ec SAE DD Hypoxia, Duty HannaDocument16 pagesMuhammad Nur, Penkes Ec SAE DD Hypoxia, Duty HannaHanna GustinPas encore d'évaluation
- Mushthafa, Penkes CB Hyponatremia DD SAE, Duty HannaDocument17 pagesMushthafa, Penkes CB Hyponatremia DD SAE, Duty HannaHanna GustinPas encore d'évaluation
- Febrianto, Sepsis Ec HAP, PIS, Duty HannaDocument17 pagesFebrianto, Sepsis Ec HAP, PIS, Duty HannaHanna GustinPas encore d'évaluation
- Deswita, SDA, Duty HannaDocument18 pagesDeswita, SDA, Duty HannaHanna GustinPas encore d'évaluation
- Meydiani, 53yo, HCU 02Document14 pagesMeydiani, 53yo, HCU 02Hanna GustinPas encore d'évaluation
- Post PartumDocument9 pagesPost PartumHanna GustinPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Pengaruh Pijat Bayi Terhadap Frekuensi Dan Durasi Menyusu BayiDocument11 pagesPengaruh Pijat Bayi Terhadap Frekuensi Dan Durasi Menyusu BayiIzmi NasutionPas encore d'évaluation
- Health EducationDocument8 pagesHealth EducationJamie Rose FontanillaPas encore d'évaluation
- 2018 Overview Digestive System HandoutDocument11 pages2018 Overview Digestive System HandoutdraganPas encore d'évaluation
- Guide State Local Emergency Operations Plans (Cpg1 8 1)Document21 pagesGuide State Local Emergency Operations Plans (Cpg1 8 1)ebjlPas encore d'évaluation
- The Warehouse Group Annual Report 2020Document92 pagesThe Warehouse Group Annual Report 2020Meaza Kidusan ElhamPas encore d'évaluation
- Autism and Transactional Analysis: TranscriptDocument26 pagesAutism and Transactional Analysis: TranscriptWanessa FernandesPas encore d'évaluation
- Editable CULC Application FormDocument4 pagesEditable CULC Application Formnniki9decPas encore d'évaluation
- Enrolled Nurses FADocument11 pagesEnrolled Nurses FAjoayou23Pas encore d'évaluation
- Arihant DRX Ascend Case Study PDFDocument2 pagesArihant DRX Ascend Case Study PDFsaurav.martPas encore d'évaluation
- SOP-016-Testing of LPG ResidueDocument9 pagesSOP-016-Testing of LPG ResidueAmnaKamranPas encore d'évaluation
- Med Tech LawsDocument78 pagesMed Tech LawsMarie LlanesPas encore d'évaluation
- As 3789.2-1991 Textiles For Health Care Facilities and Institutions Theatre Linen and Pre-PacksDocument9 pagesAs 3789.2-1991 Textiles For Health Care Facilities and Institutions Theatre Linen and Pre-PacksSAI Global - APACPas encore d'évaluation
- Sterile Potassium Chloride 10%, 15% and 20% W/V Concentrate For Solution For InfusionDocument1 pageSterile Potassium Chloride 10%, 15% and 20% W/V Concentrate For Solution For InfusionMatthew ParsonsPas encore d'évaluation
- Electronic Care and Needs Scale eCANSDocument2 pagesElectronic Care and Needs Scale eCANSamanda wuPas encore d'évaluation
- PSC Question BankDocument9 pagesPSC Question BankFaisal qblp100% (29)
- Top 10 Ranking Universities in West Africa 2022Document1 pageTop 10 Ranking Universities in West Africa 2022Bright OtcherePas encore d'évaluation
- Updated Nutrition Spreadsheet (With Workout Tracker)Document54 pagesUpdated Nutrition Spreadsheet (With Workout Tracker)Kit LbjPas encore d'évaluation
- RLE Module 3F Course Module and Procedure Guide 2Document7 pagesRLE Module 3F Course Module and Procedure Guide 2KaiPas encore d'évaluation
- Pre-Emplopyment RequirementsDocument2 pagesPre-Emplopyment RequirementsPatricia TorrianaPas encore d'évaluation
- Task 1 FinalDocument4 pagesTask 1 FinalAlᎥyⱥภPas encore d'évaluation
- Platelet Analysis - An Overview: HistoryDocument7 pagesPlatelet Analysis - An Overview: HistoryPieter Du Toit-EnslinPas encore d'évaluation
- Cultural Landscape An Introduction To Human Geography 11th Edition Rubenstein Solutions ManualDocument16 pagesCultural Landscape An Introduction To Human Geography 11th Edition Rubenstein Solutions Manualheathergarciafbqedgosyp100% (13)
- NPD Phase 1Document2 pagesNPD Phase 1Abdullah ZahidPas encore d'évaluation
- Deborah Falla The Role of Motor Learning and Neuroplasticity in Designing RehabilitationDocument5 pagesDeborah Falla The Role of Motor Learning and Neuroplasticity in Designing RehabilitationDago Angel Prieto PalavecinoPas encore d'évaluation
- Dunkin DonutsDocument2 pagesDunkin DonutszerpthederpPas encore d'évaluation
- Hearing Handicap Inventory For The Elderly (HHIE)Document5 pagesHearing Handicap Inventory For The Elderly (HHIE)Is GutiérrezPas encore d'évaluation
- Logistics Management Plan FormatDocument10 pagesLogistics Management Plan FormatAnna BellePas encore d'évaluation
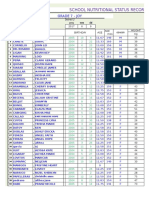
- School Nutritional Status Record: Grade 7 - JoyDocument4 pagesSchool Nutritional Status Record: Grade 7 - JoySidPas encore d'évaluation
- Objectives of The Nairobi SummitDocument12 pagesObjectives of The Nairobi SummitJoachim ChijidePas encore d'évaluation
- Quotes On StressDocument5 pagesQuotes On StressgretchhhPas encore d'évaluation