Vous aimerez peut-être aussi
- U2 All That You Can't Leave BehindDocument82 pagesU2 All That You Can't Leave BehindFranck UrsiniPas encore d'évaluation
- Factors of Active Citizenship EducationDocument2 pagesFactors of Active Citizenship EducationmauïPas encore d'évaluation
- Managerial EconomicsDocument3 pagesManagerial EconomicsGuruKPOPas encore d'évaluation
- Financial Analysis of Wipro LTDDocument101 pagesFinancial Analysis of Wipro LTDashwinchaudhary89% (18)
- National Immunization Program: Manual of Procedures Booklet 7Document32 pagesNational Immunization Program: Manual of Procedures Booklet 7Blue PielagoPas encore d'évaluation
- Guide To Raising Capital From Angel Investors Ebook From The Startup Garage PDFDocument20 pagesGuide To Raising Capital From Angel Investors Ebook From The Startup Garage PDFLars VonTurboPas encore d'évaluation
- Business Case PresentationDocument27 pagesBusiness Case Presentationapi-253435256Pas encore d'évaluation
- Microplanning For Manpower, Vaccines and Ancillary RequirementsDocument27 pagesMicroplanning For Manpower, Vaccines and Ancillary RequirementsArman BentainPas encore d'évaluation
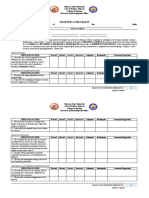
- Checklist For Thesis Chapter 3Document3 pagesChecklist For Thesis Chapter 3Richmon SantosPas encore d'évaluation
- Nip Mop Booklet 2Document42 pagesNip Mop Booklet 2Arlo Winston De GuzmanPas encore d'évaluation
- New Hire WorkbookDocument40 pagesNew Hire WorkbookkPas encore d'évaluation
- National Immunization Program: Manual of Procedures Booklet 9Document24 pagesNational Immunization Program: Manual of Procedures Booklet 9Blue PielagoPas encore d'évaluation
- GJHSP Sy 2022-2023 11292022Document64 pagesGJHSP Sy 2022-2023 11292022MERY JEAN CATACUTANPas encore d'évaluation
- School-Based Immunization MicroplanDocument3 pagesSchool-Based Immunization MicroplanicywitchPas encore d'évaluation
- Mrs. Universe PH - Empowering Women, Inspiring ChildrenDocument2 pagesMrs. Universe PH - Empowering Women, Inspiring ChildrenKate PestanasPas encore d'évaluation
- Legends and Lairs - Elemental Lore PDFDocument66 pagesLegends and Lairs - Elemental Lore PDFAlexis LoboPas encore d'évaluation
- Pre Oral ScriptDocument1 pagePre Oral Scriptcarlo maniquizPas encore d'évaluation
- Adolescent Reproductive HealthDocument218 pagesAdolescent Reproductive HealthMarissa Fontanil100% (1)
- Developing E-Module Based on Socio-Scientific Issues to Improve Students Scientific LiteracyDocument10 pagesDeveloping E-Module Based on Socio-Scientific Issues to Improve Students Scientific LiteracyTomi putra wijayaPas encore d'évaluation
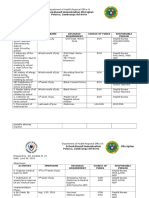
- Arh Action Plan With AcrDocument5 pagesArh Action Plan With AcrEllen Mae Cruz100% (1)
- National Immunization Program: Manual of Procedures Booklet 11Document42 pagesNational Immunization Program: Manual of Procedures Booklet 11Blue PielagoPas encore d'évaluation
- Department of Education: Republic of The PhilippinesDocument7 pagesDepartment of Education: Republic of The PhilippinesKrisha Kashmir JosePas encore d'évaluation
- Project Busog... Malusog Project Proposal 2023Document5 pagesProject Busog... Malusog Project Proposal 2023Vanessa Joy P. UrbinaPas encore d'évaluation
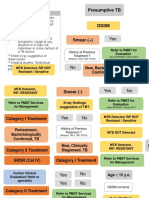
- Flowchart TB DOTSDocument11 pagesFlowchart TB DOTSalfredtan6288Pas encore d'évaluation
- Implementing Mechanism For EO 141 Presentation For NGAs - Asof15July 1 2Document35 pagesImplementing Mechanism For EO 141 Presentation For NGAs - Asof15July 1 2Reyan ArintoPas encore d'évaluation
- National Rabies Control and Prevention ProgramDocument4 pagesNational Rabies Control and Prevention Programsarguss14100% (4)
- Pulot Elementary School Implementation Plan For Ok Sa DepedDocument1 pagePulot Elementary School Implementation Plan For Ok Sa Depedmarian buenafePas encore d'évaluation
- Lewis Corporation Case 6-2 - Group 5Document8 pagesLewis Corporation Case 6-2 - Group 5Om Prakash100% (1)
- Catch-Up Ri Immunization Activity MicroplanDocument1 pageCatch-Up Ri Immunization Activity MicroplanFima JandulPas encore d'évaluation
- Detailed Lesson Plan (DLP) FormatDocument46 pagesDetailed Lesson Plan (DLP) Formatruna ylananPas encore d'évaluation
- 4 Influencing Factors of Learners Career Choice Parents Choice Vs Personal DescisionDocument24 pages4 Influencing Factors of Learners Career Choice Parents Choice Vs Personal Descisionmatteo mamaloPas encore d'évaluation
- Batangas State University Parental Consent FormDocument1 pageBatangas State University Parental Consent FormGillian Lei Carandang SacisPas encore d'évaluation
- FHSIS Report for Kitcharao Municipality in 2019Document26 pagesFHSIS Report for Kitcharao Municipality in 2019Daisy Joy MBardz100% (1)
- SIA GuidelinesDocument18 pagesSIA Guidelinestamtam06100% (1)
- Classroom Intervention Planning Sheet: Case InformationDocument1 pageClassroom Intervention Planning Sheet: Case InformationKrizzle Jane PaguelPas encore d'évaluation
- ANNUAL GENDER AND DEVELOPMENT Plan and BudgetDocument5 pagesANNUAL GENDER AND DEVELOPMENT Plan and Budgetarlene contreras-san antonioPas encore d'évaluation
- PHY210 Mechanism Ii and Thermal Physics Lab Report: Faculty of Applied Sciences Uitm Pahang (Jengka Campus)Document13 pagesPHY210 Mechanism Ii and Thermal Physics Lab Report: Faculty of Applied Sciences Uitm Pahang (Jengka Campus)Arissa SyaminaPas encore d'évaluation
- Narrative Report On Health ProtocolDocument2 pagesNarrative Report On Health ProtocolMaria Cristina Belen Reyes100% (1)
- DRRM Orientation and Coordination Meeting Private SchoolsDocument54 pagesDRRM Orientation and Coordination Meeting Private Schoolsecardnyl25Pas encore d'évaluation
- School Based Immunization-FinalDocument22 pagesSchool Based Immunization-FinalMohammed T. Abdul Razak100% (2)
- School DRRM Plan 2015Document12 pagesSchool DRRM Plan 2015Sidney Mark Animos100% (1)
- Rabies Prevention and Control ProgramDocument2 pagesRabies Prevention and Control ProgramMercurial AssasinPas encore d'évaluation
- Tuberculosis For Dec 1Document23 pagesTuberculosis For Dec 1Tony Rose Reataza-BaylonPas encore d'évaluation
- DOH School Vaccination Program Provides Lifetime ImmunityDocument28 pagesDOH School Vaccination Program Provides Lifetime ImmunityDarell Paguel Permato70% (10)
- Accomplishment Report MAR 2021Document2 pagesAccomplishment Report MAR 2021lor roaPas encore d'évaluation
- Contingency Plan For FireDocument1 pageContingency Plan For FireBachrul Ulum100% (2)
- SCHOOL HEALTH Guidelines FOR CovidDocument2 pagesSCHOOL HEALTH Guidelines FOR CovidCatherine100% (5)
- Yuhom Bacolod - Radyo Eskwela (RBI Pilot Test Brief) PDFDocument6 pagesYuhom Bacolod - Radyo Eskwela (RBI Pilot Test Brief) PDFVictoria Beltran SubaranPas encore d'évaluation
- Department of Education: Republic of The PhilippinesDocument5 pagesDepartment of Education: Republic of The PhilippinesMac Alvin GarciaPas encore d'évaluation
- USING SEODocument3 pagesUSING SEOZYNNELPas encore d'évaluation
- Case Analysis - DOH GP ProgramDocument3 pagesCase Analysis - DOH GP ProgramRobxn GrciaPas encore d'évaluation
- Gov Liezl Victoria F. PanisDocument21 pagesGov Liezl Victoria F. PanisAiza ConchadaPas encore d'évaluation
- 2017 Pds GuidelinesDocument4 pages2017 Pds GuidelinesManuel J. Degyan75% (4)
- Sample Research Instrument TemplateDocument5 pagesSample Research Instrument TemplateJomarc Cedrick GonzalesPas encore d'évaluation
- I Leadership and GovernanceDocument4 pagesI Leadership and GovernanceClerica RealingoPas encore d'évaluation
- Narrative Report: Polio Outbreak Response Immunization Bopv Round 2Document4 pagesNarrative Report: Polio Outbreak Response Immunization Bopv Round 2Cristina MelloriaPas encore d'évaluation
- Back To School Let A Million Flower Bloom ProjectDocument4 pagesBack To School Let A Million Flower Bloom ProjectPatudan ESPas encore d'évaluation
- Mental Health Care ProgramDocument8 pagesMental Health Care ProgramFibi Gwiin Polet CuanasPas encore d'évaluation
- Region V/D I V I S I O N Nutrition Model Workshop ReportDocument10 pagesRegion V/D I V I S I O N Nutrition Model Workshop Reportsalve parfiles100% (2)
- Project Proposal For Janitorial SuppliesDocument2 pagesProject Proposal For Janitorial SuppliesAngelica ObregonPas encore d'évaluation
- School Plans Cover Three YearsDocument24 pagesSchool Plans Cover Three YearsRainiel Victor M. CrisologoPas encore d'évaluation
- Plan For Vector Control Measures: Lauis National High SchoolDocument1 pagePlan For Vector Control Measures: Lauis National High SchoolIrvin EcalnirPas encore d'évaluation
- Midwives' Level of Acceptance Towards CPD Activities in GuimarasDocument43 pagesMidwives' Level of Acceptance Towards CPD Activities in GuimarasFhikery ArdientePas encore d'évaluation
- Deworming PermitDocument1 pageDeworming PermitAlvin Wilfred Ogot100% (1)
- Liquidation Forms 2021 - TarpaulinDocument21 pagesLiquidation Forms 2021 - TarpaulinKatherine DahangPas encore d'évaluation
- Catch Up Fridays AttendanceDocument6 pagesCatch Up Fridays AttendanceGladys CarreonPas encore d'évaluation
- School Immunization Campaign GuideDocument20 pagesSchool Immunization Campaign GuideHayzell Joy Fontanilla GabiPas encore d'évaluation
- Community Health Nursing (Learning Feedback Diary (LFD #25)Document3 pagesCommunity Health Nursing (Learning Feedback Diary (LFD #25)Angelica Malacay RevilPas encore d'évaluation
- School Immunization Campaign Protects Students & CommunityDocument18 pagesSchool Immunization Campaign Protects Students & CommunityDarell Paguel PermatoPas encore d'évaluation
- Childhood ImmunizationDocument16 pagesChildhood ImmunizationApple Grace TalamonPas encore d'évaluation
- SBI Deped Batangas 8 8 19Document38 pagesSBI Deped Batangas 8 8 19Lee-Ann ZerimarPas encore d'évaluation
- Technical Manual - C&C08 Digital Switching System Chapter 2 OverviewDocument19 pagesTechnical Manual - C&C08 Digital Switching System Chapter 2 OverviewSamuel100% (2)
- Journals OREF Vs ORIF D3rd RadiusDocument9 pagesJournals OREF Vs ORIF D3rd RadiusironPas encore d'évaluation
- Mounting InstructionDocument1 pageMounting InstructionAkshay GargPas encore d'évaluation
- White Box Testing Techniques: Ratna SanyalDocument23 pagesWhite Box Testing Techniques: Ratna SanyalYogesh MundhraPas encore d'évaluation
- Vector 4114NS Sis TDSDocument2 pagesVector 4114NS Sis TDSCaio OliveiraPas encore d'évaluation
- DOE Tank Safety Workshop Presentation on Hydrogen Tank TestingDocument36 pagesDOE Tank Safety Workshop Presentation on Hydrogen Tank TestingAlex AbakumovPas encore d'évaluation
- Felizardo C. Lipana National High SchoolDocument3 pagesFelizardo C. Lipana National High SchoolMelody LanuzaPas encore d'évaluation
- Todo Matic PDFDocument12 pagesTodo Matic PDFSharrife JPas encore d'évaluation
- Wheeled Loader L953F Specifications and DimensionsDocument1 pageWheeled Loader L953F Specifications and Dimensionssds khanhPas encore d'évaluation
- Test Bank For Fundamental Financial Accounting Concepts 10th by EdmondsDocument18 pagesTest Bank For Fundamental Financial Accounting Concepts 10th by Edmondsooezoapunitory.xkgyo4100% (47)
- SBI Sample PaperDocument283 pagesSBI Sample Paperbeintouch1430% (1)
- October 2009 Centeral Aucland, Royal Forest and Bird Protecton Society NewsletterDocument8 pagesOctober 2009 Centeral Aucland, Royal Forest and Bird Protecton Society NewsletterRoyal Forest and Bird Protecton SocietyPas encore d'évaluation
- EIRA v0.8.1 Beta OverviewDocument33 pagesEIRA v0.8.1 Beta OverviewAlexQuiñonesNietoPas encore d'évaluation
- Paper SizeDocument22 pagesPaper SizeAlfred Jimmy UchaPas encore d'évaluation
- Rubric 5th GradeDocument2 pagesRubric 5th GradeAlbert SantosPas encore d'évaluation
- Methods to estimate stakeholder views of sustainabilityDocument7 pagesMethods to estimate stakeholder views of sustainabilityAlireza FatemiPas encore d'évaluation
- CS709 HandoutsDocument117 pagesCS709 HandoutsalexPas encore d'évaluation
- Shopping Mall: Computer Application - IiiDocument15 pagesShopping Mall: Computer Application - IiiShadowdare VirkPas encore d'évaluation