Vous aimerez peut-être aussi
- The Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionD'EverandThe Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionPas encore d'évaluation
- Acute Renal FailureDocument30 pagesAcute Renal FailureJerinPas encore d'évaluation
- Ascites, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandAscites, A Simple Guide To The Condition, Treatment And Related ConditionsPas encore d'évaluation
- Acute Renal FailureDocument20 pagesAcute Renal FailureRufus RajPas encore d'évaluation
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesD'EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesPas encore d'évaluation
- CKD NotesDocument11 pagesCKD NotesMaria WibawaPas encore d'évaluation
- Easy Renal Diet Cookbook: Ultimate Guide To Manage Kidney DiseaseD'EverandEasy Renal Diet Cookbook: Ultimate Guide To Manage Kidney DiseasePas encore d'évaluation
- MNT Penyakit GinjalDocument41 pagesMNT Penyakit GinjalNurfitriana DwiPas encore d'évaluation
- Hepatorenal Syndrome: Causes, Tests, and Treatment OptionsD'EverandHepatorenal Syndrome: Causes, Tests, and Treatment OptionsÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)
- Acuterenalfailure2filesmerged 190509071023Document85 pagesAcuterenalfailure2filesmerged 190509071023ellise abundoPas encore d'évaluation
- The No-Salt, Lowest-Sodium Light Meals Book: Delicious Soup, Salad and Sandwich Recipes to Delight Not Only Heart and Hypertension Patients But Their Doctors as WellD'EverandThe No-Salt, Lowest-Sodium Light Meals Book: Delicious Soup, Salad and Sandwich Recipes to Delight Not Only Heart and Hypertension Patients But Their Doctors as WellÉvaluation : 5 sur 5 étoiles5/5 (1)
- Alteration in Urinary System - ppt22222Document117 pagesAlteration in Urinary System - ppt22222yen1988Pas encore d'évaluation
- End Stage Renal Disease (ESRD)Document39 pagesEnd Stage Renal Disease (ESRD)siarahPas encore d'évaluation
- Liver Curs 2009Document215 pagesLiver Curs 2009Mohammad_Islam87Pas encore d'évaluation
- Acute Renal Failure SymptomsDocument10 pagesAcute Renal Failure SymptomsEdwin Delos Reyes AbuPas encore d'évaluation
- CRFDocument50 pagesCRFKevin MontoyaPas encore d'évaluation
- Fluid Volume ExcessDocument34 pagesFluid Volume ExcessajPas encore d'évaluation
- Diseases of Urinary SystemDocument39 pagesDiseases of Urinary SystemRupak PandeyPas encore d'évaluation
- Approach To Patient With Diseases of The Kidney and Urinary Tract FINALDocument9 pagesApproach To Patient With Diseases of The Kidney and Urinary Tract FINALgelskPas encore d'évaluation
- Fluid Electrolyte Imbalance n132 160210135651Document100 pagesFluid Electrolyte Imbalance n132 160210135651Shahan FarooqPas encore d'évaluation
- Renal Disorders, Renal Failure, & Renal Dialysis: Remerose C. Ragasa, R.NDocument41 pagesRenal Disorders, Renal Failure, & Renal Dialysis: Remerose C. Ragasa, R.NremerosePas encore d'évaluation
- AscitesDocument46 pagesAscitesRahul Kumar VermaPas encore d'évaluation
- Rine Analysis: Dr. Ola Samir Ziara Modified by Dr. Amal Al MaqadmaDocument39 pagesRine Analysis: Dr. Ola Samir Ziara Modified by Dr. Amal Al Maqadmaiman zainuddinPas encore d'évaluation
- Interpretive Summary: Blood Urea Nitrogen (BUN)Document3 pagesInterpretive Summary: Blood Urea Nitrogen (BUN)Wael SafwatPas encore d'évaluation
- Cirrhosis Copy FINAL EDITEDDocument42 pagesCirrhosis Copy FINAL EDITEDpraisidPas encore d'évaluation
- Pathophysiology, Diagnosis and Treatment of Ascites in CirrhosisDocument9 pagesPathophysiology, Diagnosis and Treatment of Ascites in CirrhosisPraschyapong SamanaPas encore d'évaluation
- Diagnostic Evaluation:ARF: Changes in UrineDocument2 pagesDiagnostic Evaluation:ARF: Changes in UrineAnusha VerghesePas encore d'évaluation
- Acute Renal Failure & Chronic Renal FailureDocument38 pagesAcute Renal Failure & Chronic Renal FailureArti GondPas encore d'évaluation
- Triakoso - Urinary Tracts DisordersDocument79 pagesTriakoso - Urinary Tracts DisordersYulistia FadhilahPas encore d'évaluation
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document44 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)NaomiFettyPas encore d'évaluation
- Chronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisDocument6 pagesChronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisKyle Ü D. CunanersPas encore d'évaluation
- Etiologies of Chronic Liver Disease: Infections, Esp. Viral Toxins Genetic Drugs Autoimmune Vascular BiliaryDocument36 pagesEtiologies of Chronic Liver Disease: Infections, Esp. Viral Toxins Genetic Drugs Autoimmune Vascular BiliaryDini Permata SariPas encore d'évaluation
- Renal Calculi Concept Map PathophysiologyDocument3 pagesRenal Calculi Concept Map PathophysiologySharon TanveerPas encore d'évaluation
- Acute Kidney InjuryDocument23 pagesAcute Kidney InjuryBaraka SayorePas encore d'évaluation
- Fluid Electrolyte Balances and ImbalanceDocument157 pagesFluid Electrolyte Balances and ImbalanceManisha Shakya0% (1)
- Common ElectrolyteDocument48 pagesCommon ElectrolytemekuriawPas encore d'évaluation
- Rta Final Year 23.2.23Document36 pagesRta Final Year 23.2.23S.ayesh HasanPas encore d'évaluation
- Acute Renal FailureDocument20 pagesAcute Renal Failurewilfridus erikPas encore d'évaluation
- Abdominal Sweliing and AscitesDocument72 pagesAbdominal Sweliing and AscitesFernando Aniban100% (1)
- Hyperparathyroidsm HANDOUTDocument2 pagesHyperparathyroidsm HANDOUTmendellianPas encore d'évaluation
- Renal Calculi: Urolithiasis, Nephrolithiasis, Renal StoneDocument18 pagesRenal Calculi: Urolithiasis, Nephrolithiasis, Renal StonerohitPas encore d'évaluation
- Fluids and ElectrolytesDocument19 pagesFluids and Electrolytesderic100% (5)
- Urine Analysis FinalDocument112 pagesUrine Analysis FinalNischita JayarajPas encore d'évaluation
- Problems With Sodium and PotassiumDocument34 pagesProblems With Sodium and PotassiumJemima Nove JapitanaPas encore d'évaluation
- Alteration in Fluid and Electrolyte ImbalanceDocument118 pagesAlteration in Fluid and Electrolyte ImbalanceRenuga SureshPas encore d'évaluation
- Stones in The BodyDocument14 pagesStones in The BodyMichaelPas encore d'évaluation
- Sistem UrinariaDocument42 pagesSistem UrinariaHanny da GamaPas encore d'évaluation
- Hyper Ure Semi ADocument44 pagesHyper Ure Semi Abagusputrabali13Pas encore d'évaluation
- Acute Chronic Kidney InjuryDocument29 pagesAcute Chronic Kidney InjuryPriya GKPas encore d'évaluation
- Genito Urinary SystemDocument106 pagesGenito Urinary Systemnursereview88% (8)
- Renal SystemDocument20 pagesRenal SystemRahul DasPas encore d'évaluation
- Acute Kidney InjuryDocument60 pagesAcute Kidney InjuryAbegail Fermanejo-GeneraoPas encore d'évaluation
- Genitourinary DisordersDocument2 pagesGenitourinary DisordersGwenn SalazarPas encore d'évaluation
- CKD - For Concept MappingDocument7 pagesCKD - For Concept MappingKennette Lim0% (1)
- GenitoUrinary Tract PresentationDocument60 pagesGenitoUrinary Tract PresentationJaezee RamosPas encore d'évaluation
- Uric Acid Determination PDFDocument10 pagesUric Acid Determination PDFJhon Jerome DapdapPas encore d'évaluation
- Pathophysiology - The LiverDocument66 pagesPathophysiology - The LiverMichelle BilayaPas encore d'évaluation
- Water & Electrolyte BalanceDocument27 pagesWater & Electrolyte Balanceanisa rachmitaPas encore d'évaluation
- Mia Treatment Guidelines 2007Document39 pagesMia Treatment Guidelines 2007楊將群Pas encore d'évaluation
- Fluid & Electrolyte, Acid-Base Imbalance (MS REPORT)Document41 pagesFluid & Electrolyte, Acid-Base Imbalance (MS REPORT)Jane BelvisPas encore d'évaluation
- Case Study of Liver CirrhosisDocument3 pagesCase Study of Liver Cirrhosisbuzz Q100% (1)
- ReadmeDocument1 pageReadmebuzz QPas encore d'évaluation
- Case Study of LeptospirosisDocument4 pagesCase Study of Leptospirosisbuzz Q75% (4)
- Case Study of DMDocument6 pagesCase Study of DMbuzz Q0% (1)
- Musical InstrumentsDocument12 pagesMusical Instrumentsbuzz QPas encore d'évaluation
- Case Study of AmoebiasisDocument7 pagesCase Study of Amoebiasisbuzz Q75% (4)
- Case Study of AsthmaDocument6 pagesCase Study of Asthmabuzz Q100% (4)
- RespiratoryDocument249 pagesRespiratorybuzz Q100% (3)
- Assessment Slide ShowDocument144 pagesAssessment Slide Showbuzz QPas encore d'évaluation
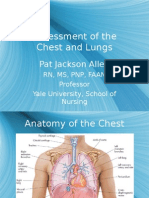
- Assessment of The Chest and Lungs: Pat Jackson AllenDocument50 pagesAssessment of The Chest and Lungs: Pat Jackson Allenbuzz Q100% (3)
- AbdomenDocument100 pagesAbdomenbuzz Q83% (6)
- Phobia ListDocument48 pagesPhobia Listbuzz QPas encore d'évaluation
- CardiovascularDocument122 pagesCardiovascularbuzz QPas encore d'évaluation
- Assessment of The Skin: Pat Jackson AllenDocument104 pagesAssessment of The Skin: Pat Jackson Allenbuzz Q100% (4)
- The Reproductive SystemDocument18 pagesThe Reproductive Systembuzz QPas encore d'évaluation
- The Pulmonary SystemDocument21 pagesThe Pulmonary Systembuzz QPas encore d'évaluation
- UrologyDocument28 pagesUrologybuzz QPas encore d'évaluation
- Care of The NewbornDocument5 pagesCare of The Newbornbuzz Q100% (2)
- Growth and DevelopmentDocument6 pagesGrowth and Developmentbuzz Q100% (3)
- The Cardiovascular SystemDocument20 pagesThe Cardiovascular Systembuzz QPas encore d'évaluation
- Musculoskeletal SystemDocument50 pagesMusculoskeletal Systembuzz QPas encore d'évaluation
- SensesDocument44 pagesSensesbuzz Q100% (1)
- NeurologyDocument42 pagesNeurologybuzz Q100% (2)
- Digestive SystemDocument38 pagesDigestive Systembuzz QPas encore d'évaluation
- DermaDocument33 pagesDermabuzz QPas encore d'évaluation
- ImmunologyDocument23 pagesImmunologybuzz QPas encore d'évaluation
- Basic ChemistryDocument47 pagesBasic Chemistrybuzz QPas encore d'évaluation
- Abnormal Urinalysis Children-Tadulako2015Document33 pagesAbnormal Urinalysis Children-Tadulako2015Yeyen Hastriam AkramPas encore d'évaluation
- @acute Nephritic SyndromeDocument3 pages@acute Nephritic SyndromeMazlia FarzanaPas encore d'évaluation
- Krok2 - Medicine - 2010Document27 pagesKrok2 - Medicine - 2010Badriya YussufPas encore d'évaluation
- Multiple Choice Questions: C Minimal-Change NephropathyDocument3 pagesMultiple Choice Questions: C Minimal-Change NephropathyIM CT50% (2)
- MKSAP 19 (Medical Knowledge Self-Assessment Program) Nephrology (American College of Physicians) (American College of Physicians)Document195 pagesMKSAP 19 (Medical Knowledge Self-Assessment Program) Nephrology (American College of Physicians) (American College of Physicians)Emin bojecPas encore d'évaluation
- Pathology B - Midterm Ratio: Prelim TopicsDocument69 pagesPathology B - Midterm Ratio: Prelim TopicsHuey Manalang JavierPas encore d'évaluation
- Pathology Ple SamplexDocument5 pagesPathology Ple SamplexdawnparkPas encore d'évaluation
- Nephritic Syndrome - ScienceDirectDocument5 pagesNephritic Syndrome - ScienceDirectraul.villarrealPas encore d'évaluation
- RenalDocument81 pagesRenalandreaPas encore d'évaluation
- Genpath - Glomerular Diseases (Primary Glomerulopathies (Nephritic) )Document5 pagesGenpath - Glomerular Diseases (Primary Glomerulopathies (Nephritic) )Julie Gemarino LumasagPas encore d'évaluation
- Renal BiopsyDocument19 pagesRenal BiopsyPriyank GuptaPas encore d'évaluation
- Pathology MUHS Questions (2005-2015)Document5 pagesPathology MUHS Questions (2005-2015)Shahid KhanPas encore d'évaluation
- Benign Familial HematuriaDocument6 pagesBenign Familial Hematuriasiska_mariannaPas encore d'évaluation
- Genitourinary Tract InfectionsDocument80 pagesGenitourinary Tract Infectionsraene_bautistaPas encore d'évaluation
- Amharic ConversationDocument94 pagesAmharic Conversationtsehay asratPas encore d'évaluation
- Nephrotic and Nephritic Syndrome - 2008Document65 pagesNephrotic and Nephritic Syndrome - 2008rikasusanti101001201Pas encore d'évaluation
- PathologyDocument30 pagesPathologyTenorski baritonPas encore d'évaluation
- Renal Pathology Lectures - PPT SeriesDocument267 pagesRenal Pathology Lectures - PPT SeriesMarc Imhotep Cray, M.D.100% (12)
- AbbreviationDocument19 pagesAbbreviationJayson NatividadPas encore d'évaluation
- STG - ETHIPIA 2020 PDF With Clickable TOCDocument1 222 pagesSTG - ETHIPIA 2020 PDF With Clickable TOCMihretPas encore d'évaluation
- Nephrotic SyndromeDocument21 pagesNephrotic Syndromepreetie8750% (4)
- IVMS Comprehensive Pathology Examination W AnswersDocument55 pagesIVMS Comprehensive Pathology Examination W AnswersMarc Imhotep Cray, M.D.100% (4)
- Biomarkers in Progressive Chronic Kidney Disease. Still A Long Way To GoDocument13 pagesBiomarkers in Progressive Chronic Kidney Disease. Still A Long Way To GoconstanzanazarethPas encore d'évaluation
- The Columbia Renal Biopsy Course: JULY 12 - JULY 14, 2023Document8 pagesThe Columbia Renal Biopsy Course: JULY 12 - JULY 14, 2023Freddy Shanner Chávez VásquezPas encore d'évaluation
- Atlas Urinary Sediments Renal BiopsiesDocument8 pagesAtlas Urinary Sediments Renal BiopsiesiruntoroPas encore d'évaluation
- Nephrotic and Nephritic SyndromesDocument27 pagesNephrotic and Nephritic SyndromesJoshua Smith100% (1)
- Nephrotic and Nephritic - SyndromeDocument35 pagesNephrotic and Nephritic - SyndromeadinayPas encore d'évaluation
- Case 2Document4 pagesCase 2Kim Ruiz100% (1)
- Pediatrics BookDocument53 pagesPediatrics BookMobin Ur Rehman Khan100% (1)
- Nephrology MRCP1Document174 pagesNephrology MRCP1Raouf Ra'fat Soliman100% (3)