Vous aimerez peut-être aussi
- Skills Building Maternal and Child Care: Prepared By: Angeli Joy V. MontonDocument61 pagesSkills Building Maternal and Child Care: Prepared By: Angeli Joy V. MontonboinkjilijoyPas encore d'évaluation
- (备份)皇冠GRE新新高高频填空篇(2022版) pdf 20231025201907593Document167 pages(备份)皇冠GRE新新高高频填空篇(2022版) pdf 20231025201907593florexxi19Pas encore d'évaluation
- Respironics V60 Users ManualDocument160 pagesRespironics V60 Users ManualAnonymous pzadxGS2CNPas encore d'évaluation
- Stages and Mechanism of LaborDocument14 pagesStages and Mechanism of LaborRhea Jane BongcatoPas encore d'évaluation
- Stages of LaborDocument23 pagesStages of LaborPortia Dulce Toquero100% (5)
- Complete Mind FullDocument1 079 pagesComplete Mind FullhayasakaPas encore d'évaluation
- Stages of LaborDocument19 pagesStages of LaborDumlao JellyPas encore d'évaluation
- The Positive Influence of Peer Pressure To Education StudentsDocument15 pagesThe Positive Influence of Peer Pressure To Education StudentsDaniela GalinganPas encore d'évaluation
- Stages of Labor: Dela Cruz, Dineros, DimaporoDocument25 pagesStages of Labor: Dela Cruz, Dineros, DimaporoEvelyn MedinaPas encore d'évaluation
- Birth: Labor & Caesarian SectionDocument31 pagesBirth: Labor & Caesarian SectionAGLDPas encore d'évaluation
- Stages of LaborDocument51 pagesStages of LaborZeen_Zeen_Fern_3128100% (4)
- Management of Normal LaborDocument37 pagesManagement of Normal LaborSilvestri Purba100% (1)
- HSE Lecture NotesDocument10 pagesHSE Lecture NotesAndrePas encore d'évaluation
- Labor and Delivery - 1Document32 pagesLabor and Delivery - 1Lauren TrenchardPas encore d'évaluation
- Ob Case Study FinalDocument18 pagesOb Case Study FinalAlthea Mchanes100% (2)
- Stages of LaborDocument3 pagesStages of LaborFelmerPolancoRodaPas encore d'évaluation
- Physiology and Management of 1St Stage of LabourDocument5 pagesPhysiology and Management of 1St Stage of LabourSucharita PandaPas encore d'évaluation
- McGrath MAC Video Laryngoscope Instructions For Use PDFDocument24 pagesMcGrath MAC Video Laryngoscope Instructions For Use PDFAnonymous MnaMZQWwCPas encore d'évaluation
- Labor & DeliveryDocument28 pagesLabor & DeliveryVenice Joy Toledo-Malonzo,RN100% (1)
- Bioethics Session 16 SASDocument4 pagesBioethics Session 16 SASAnthony BadiliPas encore d'évaluation
- The Final Trimester: A Guide to Everything to Expect in the Third Trimester of Pregnancy and ChildbirthD'EverandThe Final Trimester: A Guide to Everything to Expect in the Third Trimester of Pregnancy and ChildbirthÉvaluation : 5 sur 5 étoiles5/5 (1)
- Level of Knowledge and Attitude Among Nursing Students Toward Patient Safety and Medical ErrorsDocument125 pagesLevel of Knowledge and Attitude Among Nursing Students Toward Patient Safety and Medical ErrorshanadiPas encore d'évaluation
- Management of The First Stage of Labour LectureDocument48 pagesManagement of The First Stage of Labour LectureJSeashark100% (3)
- 15 Signs Stages of LaborDocument84 pages15 Signs Stages of LaborDorothy Jane OrdinarioPas encore d'évaluation
- mh6zxph8r - 11 STAGES - OF - LABORDocument25 pagesmh6zxph8r - 11 STAGES - OF - LABORHecy CristoPas encore d'évaluation
- Normal Labour and Birth UohDocument148 pagesNormal Labour and Birth UohCaamir Dek HaybePas encore d'évaluation
- Normal Labour and Birth Uoh 2023Document159 pagesNormal Labour and Birth Uoh 2023Caamir Dek HaybePas encore d'évaluation
- Crisanto Cajang Mariecor Enriquez Kathleen Jayne Ramos Kathleen Kayla Baguioen Rosemarie Joy JucutanDocument58 pagesCrisanto Cajang Mariecor Enriquez Kathleen Jayne Ramos Kathleen Kayla Baguioen Rosemarie Joy JucutanGary PicarPas encore d'évaluation
- Labor and DeliveryDocument22 pagesLabor and DeliveryClyde CapadnganPas encore d'évaluation
- OB Stages of Labor and Care in The Stages of Labor With VideoDocument45 pagesOB Stages of Labor and Care in The Stages of Labor With VideodsmagallanesPas encore d'évaluation
- Intra Partal Care To Post Partal CareDocument174 pagesIntra Partal Care To Post Partal CareBriana Louise HernandezPas encore d'évaluation
- Normal Labour July 2013Document13 pagesNormal Labour July 2013Logan MakolaPas encore d'évaluation
- Normal Spontaneous Delivery: Reyes, Janyn Marione ADocument35 pagesNormal Spontaneous Delivery: Reyes, Janyn Marione AJanyn Abella ReyesPas encore d'évaluation
- Stages of LaborDocument3 pagesStages of LaborCleo Pabilic100% (1)
- Updated NCM 107 Lecture Week 7Document27 pagesUpdated NCM 107 Lecture Week 7Quencee CalaycayPas encore d'évaluation
- 1st and 2nd Stage of LabourDocument137 pages1st and 2nd Stage of Labournixon odoyoPas encore d'évaluation
- Labour Presentation ObsDocument48 pagesLabour Presentation ObsVera BannorPas encore d'évaluation
- Stages of Labor & Leopold's Maneuver First Stage: Dilating StageDocument11 pagesStages of Labor & Leopold's Maneuver First Stage: Dilating StagePanJan BalPas encore d'évaluation
- Final MCNDocument3 pagesFinal MCNKyla R. PinedaPas encore d'évaluation
- Stages of LaborDocument11 pagesStages of LaborE=MC2Pas encore d'évaluation
- Teaching Module LaborDocument28 pagesTeaching Module LabordrsikandarPas encore d'évaluation
- Labor DeliveryDocument28 pagesLabor DeliveryJenica ManuntagPas encore d'évaluation
- Conduct of Normal Labor - Ivan Paul ValdezDocument31 pagesConduct of Normal Labor - Ivan Paul ValdezLouis Carlos RoderosPas encore d'évaluation
- Labor and Birth (Part3)Document37 pagesLabor and Birth (Part3)Nayef AlsalmiPas encore d'évaluation
- Labor and Delivery ConceptsDocument8 pagesLabor and Delivery ConceptsNisah CabugatanPas encore d'évaluation
- Stages of Normal Labor - PTXDocument8 pagesStages of Normal Labor - PTXMacMacPas encore d'évaluation
- LaborDocument45 pagesLaborDakayu Amin LugitPas encore d'évaluation
- Normal Labour 400lDocument102 pagesNormal Labour 400lAbdullahi Suleiman MakaPas encore d'évaluation
- Management of First Stage of LabourDocument35 pagesManagement of First Stage of LabourPragati BholePas encore d'évaluation
- Stages of Labor & Delivery and Danger Signs of Labor: Week 11 ReportersDocument30 pagesStages of Labor & Delivery and Danger Signs of Labor: Week 11 ReportersMushy_ayaPas encore d'évaluation
- Stages of LaborDocument3 pagesStages of LaborJepoy GomezPas encore d'évaluation
- Chapter 15 (Part 2) Caring For A Woman During Vaginal Birth: Cardinal Movements of LaborDocument7 pagesChapter 15 (Part 2) Caring For A Woman During Vaginal Birth: Cardinal Movements of Labor3amabelle arevaloPas encore d'évaluation
- Normal Labor and DeliveryDocument77 pagesNormal Labor and DeliveryLouis Carlos RoderosPas encore d'évaluation
- Intrapartal Period: Methods of Pain ManagementDocument7 pagesIntrapartal Period: Methods of Pain Managementdarkscaler100% (2)
- Stage 1Document10 pagesStage 1JosephNawenPas encore d'évaluation
- Labor: District 1 ACOG Medical Student Education Module 2008Document28 pagesLabor: District 1 ACOG Medical Student Education Module 2008Gabriel ZuñigaPas encore d'évaluation
- MaternalDocument6 pagesMaternalNorbelisa Tabo-ac CadungganPas encore d'évaluation
- Stages of LaborDocument16 pagesStages of LaborThrecia RotaPas encore d'évaluation
- Maternal NewbornDocument49 pagesMaternal NewbornEve Marie FernandezPas encore d'évaluation
- Laboranddelivery NotesDocument6 pagesLaboranddelivery NotesStudent NursePas encore d'évaluation
- Assesment and Monitoring During 2nd Stage of LabourDocument11 pagesAssesment and Monitoring During 2nd Stage of LabourPragati BholePas encore d'évaluation
- Stages of LaborDocument3 pagesStages of LaborAndreiPas encore d'évaluation
- Intrapartum: 2 Stage of LaborDocument46 pagesIntrapartum: 2 Stage of LaborJamie Haravata100% (1)
- Regodos Stages of LaborDocument91 pagesRegodos Stages of LaborIan Cyrus RegodosPas encore d'évaluation
- Obstetric & Gynecology Nursing: Topic-Physiological Changes During LabourDocument54 pagesObstetric & Gynecology Nursing: Topic-Physiological Changes During LabourBhumi ChouhanPas encore d'évaluation
- Maternal and ChildDocument4 pagesMaternal and ChildChin Chan100% (1)
- Intrapartal - Theories of LaborDocument21 pagesIntrapartal - Theories of LaborJan Oliver YaresPas encore d'évaluation
- Stages of LaborDocument4 pagesStages of LaborAizy BastionPas encore d'évaluation
- The Seven Steps That Save Lives: Swedish VersionDocument11 pagesThe Seven Steps That Save Lives: Swedish VersionItachi SaiyanPas encore d'évaluation
- Thai Foot Reflexology With The Wooden Stick Autor Heath & Nicole ReedDocument17 pagesThai Foot Reflexology With The Wooden Stick Autor Heath & Nicole ReedAlvydas VitkauskasPas encore d'évaluation
- Limb Defciency and Phantom Limb QuestionnaireDocument5 pagesLimb Defciency and Phantom Limb Questionnairenadia kurniaPas encore d'évaluation
- VentilatorDocument15 pagesVentilatorMohamedPas encore d'évaluation
- History of NaturopathyDocument5 pagesHistory of Naturopathyglenn johnstonPas encore d'évaluation
- Legal Medicine Notes 2020Document8 pagesLegal Medicine Notes 2020Iamharbeyy CastroPas encore d'évaluation
- Legislative Counsel's Digest:: 32nd Special Session (2020)Document22 pagesLegislative Counsel's Digest:: 32nd Special Session (2020)FOX5 VegasPas encore d'évaluation
- Emirates Aluminium Smelter Complex QA PlanDocument32 pagesEmirates Aluminium Smelter Complex QA PlanSagar AliasjackeyPas encore d'évaluation
- PHYSICIANS Room Assignment 03-2021Document13 pagesPHYSICIANS Room Assignment 03-2021PRC BaguioPas encore d'évaluation
- How Does Religion Affect The Quality of Life?Document7 pagesHow Does Religion Affect The Quality of Life?Jashan Rohit KumarPas encore d'évaluation
- McKenzie CONCEPT AnilDocument12 pagesMcKenzie CONCEPT AnilSOUMYADEEP BHUINYAPas encore d'évaluation
- Mukhtar Mohamed's Cover Letter PDFDocument1 pageMukhtar Mohamed's Cover Letter PDFEng-Mukhtaar Catoosh100% (3)
- Madalynn Young Resume 2022Document1 pageMadalynn Young Resume 2022api-609263330Pas encore d'évaluation
- Kudori Therapy - Updated 9th Dec17Document32 pagesKudori Therapy - Updated 9th Dec17Manickavasagam RengarajuPas encore d'évaluation
- IARCDocument868 pagesIARCmarcosiqPas encore d'évaluation
- Practice Test A3Document8 pagesPractice Test A3Khang Nguyen TienPas encore d'évaluation
- Chapter 1 & 2 PDFDocument15 pagesChapter 1 & 2 PDF11D3 CHUA , Jasmine B.Pas encore d'évaluation
- Toxic Positivity (An Essay)Document2 pagesToxic Positivity (An Essay)Colossal HeartPas encore d'évaluation
- Leistner 2000 PDFDocument6 pagesLeistner 2000 PDFProf C.S.PurushothamanPas encore d'évaluation
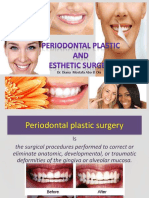
- Dr. Diana Mostafa Abo El OlaDocument68 pagesDr. Diana Mostafa Abo El Olasohaib natshehPas encore d'évaluation
- 1548 6066 1 PBDocument10 pages1548 6066 1 PBOun VikrethPas encore d'évaluation
- 2021 Anesthesia System S6100Document2 pages2021 Anesthesia System S6100Luis RodriguezPas encore d'évaluation