Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
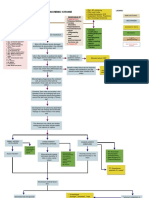
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- CVA Case PresentationDocument25 pagesCVA Case PresentationChucky VergaraPas encore d'évaluation
- CT Coronary Angiography: 256-Slice and 320-Detector Row ScannersDocument12 pagesCT Coronary Angiography: 256-Slice and 320-Detector Row ScannersCruceanu SimonaPas encore d'évaluation
- Medical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 58Document11 pagesMedical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 58sarasjunkPas encore d'évaluation
- Pathophysiology of Coronary Artery Disease: Basic Science For CliniciansDocument8 pagesPathophysiology of Coronary Artery Disease: Basic Science For CliniciansZaenal AhmadPas encore d'évaluation
- Acute Arterial OcclusionDocument39 pagesAcute Arterial Occlusionmaria teresa casili100% (1)
- 2014 @nucproflib Helen Ryder, GiorgioDocument128 pages2014 @nucproflib Helen Ryder, Giorgioe'Rfan k'AguyaPas encore d'évaluation
- Acute Coronary SyndromeDocument19 pagesAcute Coronary SyndromeSherree HayesPas encore d'évaluation
- CoronarografieDocument72 pagesCoronarografieLaurentiu AndreiPas encore d'évaluation
- Case Study3Document13 pagesCase Study3Nadine FormaranPas encore d'évaluation
- Atherosclerosis and ArteriosclerosisDocument50 pagesAtherosclerosis and ArteriosclerosisApril Carter100% (1)
- Coronarry Artery DiseaseDocument24 pagesCoronarry Artery DiseaseAriess897Pas encore d'évaluation
- Jurnal 3Document4 pagesJurnal 3Arum RaniPas encore d'évaluation
- Pathophysiology of Atherosclerosis, Thrombosis and EmbolismDocument4 pagesPathophysiology of Atherosclerosis, Thrombosis and EmbolismKeshant Samaroo100% (1)
- Guidelines For Diagnosis and Treatment of Patients With Vasospas 2014Document23 pagesGuidelines For Diagnosis and Treatment of Patients With Vasospas 2014he xuPas encore d'évaluation
- Case Study 1Document3 pagesCase Study 1Da NicaPas encore d'évaluation
- Cardiovascular DiseaseDocument5 pagesCardiovascular DiseaseJohn SammutPas encore d'évaluation
- Enzyme 20pagesDocument20 pagesEnzyme 20pagesEddie Optin100% (2)
- Cardiovascular Imaging For Clinical Practice - Nicholls e WorthleyDocument397 pagesCardiovascular Imaging For Clinical Practice - Nicholls e WorthleyStephanie ElexiasPas encore d'évaluation
- Interventional NeuroradiologyDocument8 pagesInterventional NeuroradiologyAbhinav GuptaPas encore d'évaluation
- A Bornstein, MD, FACC Assistant Professor of Public Health Weill Cornell Medical CollegeDocument50 pagesA Bornstein, MD, FACC Assistant Professor of Public Health Weill Cornell Medical CollegeSyed ImranPas encore d'évaluation
- Role of MDCT in Coronary Artery Disease: Swachchhanda Songmen 2071Document63 pagesRole of MDCT in Coronary Artery Disease: Swachchhanda Songmen 2071Dr KhanPas encore d'évaluation
- Journal of Food Biochemistry - 2022 - Rana - Health Benefits of Polyphenols A Concise ReviewDocument24 pagesJournal of Food Biochemistry - 2022 - Rana - Health Benefits of Polyphenols A Concise ReviewGustavoTorresPas encore d'évaluation
- Unit Two The Health Benefits of Physical ActivityDocument10 pagesUnit Two The Health Benefits of Physical ActivityYoseph DefaruPas encore d'évaluation
- Current Management Strategies in ACS-Intervention or Conservative - Note, Dr. Faris B, SP - JP (K) FAP PDFDocument51 pagesCurrent Management Strategies in ACS-Intervention or Conservative - Note, Dr. Faris B, SP - JP (K) FAP PDFSofia KusumadewiPas encore d'évaluation
- Atherosclerosis & Trombosis Dr. FaturochmanDocument50 pagesAtherosclerosis & Trombosis Dr. FaturochmanPutry RizqiaPas encore d'évaluation
- Basic Principles of Platelet Biology and Clinical ImplicationsDocument11 pagesBasic Principles of Platelet Biology and Clinical ImplicationsIsmael Rivera DiazPas encore d'évaluation
- LES y Enf CardiovascularDocument15 pagesLES y Enf CardiovascularSMIBA MedicinaPas encore d'évaluation
- Human Biological Science 2 BIOL122: National Workshop Manual 2019Document78 pagesHuman Biological Science 2 BIOL122: National Workshop Manual 2019Huge Lovely SmilePas encore d'évaluation
- Chap 11Document22 pagesChap 11vchan318Pas encore d'évaluation