Vous aimerez peut-être aussi
- Welcoming To Wi-Fi To Home NetworksDocument2 pagesWelcoming To Wi-Fi To Home NetworksseanpercivalPas encore d'évaluation
- Holiday ShowcaseDocument1 pageHoliday ShowcaseseanpercivalPas encore d'évaluation
- Rental ApplicationDocument2 pagesRental Applicationseanpercival100% (1)
- Ohio Academy of Family PhysiciansDocument8 pagesOhio Academy of Family PhysiciansseanpercivalPas encore d'évaluation
- Advances in Environmental MonitoringDocument17 pagesAdvances in Environmental MonitoringseanpercivalPas encore d'évaluation
- Emotional EvolutionDocument6 pagesEmotional EvolutionseanpercivalPas encore d'évaluation
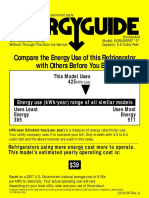
- Energy Guide To Compare RefrigeratorsDocument2 pagesEnergy Guide To Compare RefrigeratorsseanpercivalPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Chapter-3 Synthesis, Characterization of Some Novel Chromeno Oxadiazole DerivativesDocument43 pagesChapter-3 Synthesis, Characterization of Some Novel Chromeno Oxadiazole DerivativesMadalina GhitaPas encore d'évaluation
- American Journal of Infection ControlDocument5 pagesAmerican Journal of Infection ControlEileen Le RouxPas encore d'évaluation
- Anaemia in Children by Nsubuga Hamisi: Year 3 MBCHB Facilitated by Dr. Kamugisha Albert Date 29/09/2017Document38 pagesAnaemia in Children by Nsubuga Hamisi: Year 3 MBCHB Facilitated by Dr. Kamugisha Albert Date 29/09/2017NinaPas encore d'évaluation
- Module 4 KKKDocument32 pagesModule 4 KKKbhrayancacheroPas encore d'évaluation
- MCB Lab ReviewerDocument5 pagesMCB Lab ReviewerJhoanna Mae MinionPas encore d'évaluation
- TickDocument10 pagesTickmarioaPas encore d'évaluation
- Theory Part B-20.7.2016Document58 pagesTheory Part B-20.7.2016KaniyaTabinaPas encore d'évaluation
- Chapter 14 Mendel and The Gene IdeaDocument9 pagesChapter 14 Mendel and The Gene IdeaJUNG LEEPas encore d'évaluation
- Dapi SigmaDocument2 pagesDapi SigmaeliavvPas encore d'évaluation
- Evaluation of Dysuria in AdultsDocument8 pagesEvaluation of Dysuria in AdultspapermintPas encore d'évaluation
- PDQ HistoDocument225 pagesPDQ HistoHtike Myat PhyuPas encore d'évaluation
- Labcomp FDocument23 pagesLabcomp Fking peacePas encore d'évaluation
- Gene Therapy: by Prof. Liwayway Memije-CruzDocument12 pagesGene Therapy: by Prof. Liwayway Memije-CruzMarie WongPas encore d'évaluation
- ClinDermatolRev133-5811533 160835Document9 pagesClinDermatolRev133-5811533 160835rehanaPas encore d'évaluation
- Grade 11 Biology Midterm HLDocument31 pagesGrade 11 Biology Midterm HLSaima SyedaPas encore d'évaluation
- Safety and Side Effects of RifampinDocument10 pagesSafety and Side Effects of RifampinbagusPas encore d'évaluation
- CytogeneticsDocument17 pagesCytogeneticsLee LuceroPas encore d'évaluation
- A Color Atlas of Poultry Diseases by J L VegadDocument144 pagesA Color Atlas of Poultry Diseases by J L VegadId DyPas encore d'évaluation
- Introduction To FungiDocument13 pagesIntroduction To FungiYekitaSPas encore d'évaluation
- Table Atrial FlagellatesDocument4 pagesTable Atrial FlagellatesNinaRicaR.RamosPas encore d'évaluation
- Understanding Pneumonia: Causes, Symptoms, and TreatmentDocument5 pagesUnderstanding Pneumonia: Causes, Symptoms, and TreatmentrjshubhPas encore d'évaluation
- Makalah Sistem Pencernaan Bhs InggrisDocument32 pagesMakalah Sistem Pencernaan Bhs InggrisDesiPas encore d'évaluation
- BioinformaticsDocument167 pagesBioinformaticsGilbert MethewPas encore d'évaluation
- Yersinia SPP: The Black Death'Document23 pagesYersinia SPP: The Black Death'bujalkanPas encore d'évaluation
- Annexure 4 Colony Morphology, Shape & Cell Arrangment of MicroorganismDocument6 pagesAnnexure 4 Colony Morphology, Shape & Cell Arrangment of Microorganismdinesh singhPas encore d'évaluation
- Chem Soc Rev: ViewpointDocument9 pagesChem Soc Rev: Viewpointdiansapitri083Pas encore d'évaluation
- Acog Practice BulletinDocument10 pagesAcog Practice BulletinCristian AranibarPas encore d'évaluation
- Editorial: Decisions and Antibiotics Use: More Questions and Some AnswersDocument3 pagesEditorial: Decisions and Antibiotics Use: More Questions and Some AnswersTommy Leon SilvaPas encore d'évaluation
- What Is Malaria PDFDocument6 pagesWhat Is Malaria PDFtisya f raminPas encore d'évaluation
- Biopesticides For PestscontrolDocument9 pagesBiopesticides For Pestscontrolmap solutionsPas encore d'évaluation