Vous aimerez peut-être aussi
- Causes of Male InfertilityDocument31 pagesCauses of Male InfertilityChris Emmanuel NathanPas encore d'évaluation
- 3rd Stage ComplicationsDocument84 pages3rd Stage ComplicationsDream100% (1)
- Pregnancy Induced Hypertension: DefinitionDocument7 pagesPregnancy Induced Hypertension: Definitionkristine hinaresPas encore d'évaluation
- InfertilityDocument24 pagesInfertilitySimran JosanPas encore d'évaluation
- Clinical Teaching 4PEUPERAL SEPSISDocument5 pagesClinical Teaching 4PEUPERAL SEPSISAjit M Prasad Prasad100% (1)
- Partograph PPT 1Document55 pagesPartograph PPT 1Maria Lejani Terencio100% (1)
- Identifying Clients at RiskDocument57 pagesIdentifying Clients at Riskcoosa liquors100% (1)
- Anorectal Malformations: Presented by Khushveer KaurDocument91 pagesAnorectal Malformations: Presented by Khushveer KaurKataria DavinPas encore d'évaluation
- Purperal InfectionsDocument69 pagesPurperal InfectionsBeulah DasariPas encore d'évaluation
- AMNIOCENTESISDocument9 pagesAMNIOCENTESISSANCHAYEETA100% (1)
- Family PlanningDocument18 pagesFamily Planningselja0% (1)
- Obstetric Emergencies and Anesthetic Management: Co-Ordinator: DR - Navab Singh (M.D.) Speaker: Dr. UdayDocument35 pagesObstetric Emergencies and Anesthetic Management: Co-Ordinator: DR - Navab Singh (M.D.) Speaker: Dr. UdayKutumela MolebogengPas encore d'évaluation
- AbortionDocument66 pagesAbortionGunu SinghPas encore d'évaluation
- Rating Scale For The Gynecologic ExamDocument3 pagesRating Scale For The Gynecologic ExamAnonymous qJM3kLDtPas encore d'évaluation
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesD'EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesPas encore d'évaluation
- Polyhydramnios (Revised)Document34 pagesPolyhydramnios (Revised)Edward Munyaradzi KutsanziraPas encore d'évaluation
- Antenatal PreparationDocument24 pagesAntenatal PreparationSwatiPas encore d'évaluation
- LESSON PLAN ON Hyper Emesis GravidarumDocument12 pagesLESSON PLAN ON Hyper Emesis GravidarumMadhavi ModaPas encore d'évaluation
- Chapter 10 - Lexi Cowslip - HELLP SyndromeDocument7 pagesChapter 10 - Lexi Cowslip - HELLP SyndromeEunice Cortés100% (1)
- Puerperal InfectionDocument28 pagesPuerperal Infectionputri1114Pas encore d'évaluation
- IUGRDocument6 pagesIUGRabhagaurPas encore d'évaluation
- Vaginal/Cervical Examination: Cristin G. Ungab, MNDocument21 pagesVaginal/Cervical Examination: Cristin G. Ungab, MNCristin Ungab100% (1)
- Introduction To Pediatric NursingDocument36 pagesIntroduction To Pediatric Nursingcharan poonia100% (1)
- Lymphoma in ChildrenDocument42 pagesLymphoma in ChildrenPriyaPas encore d'évaluation
- Normal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, VapiDocument48 pagesNormal Labor: Ms. Mayuri Patel Sandra Shroff Rofel College of Nursing, Vapivimmy47100% (1)
- Active Management of 3RD Stage of LaborDocument7 pagesActive Management of 3RD Stage of LaborFarheen khanPas encore d'évaluation
- WelcomeDocument103 pagesWelcomeLyka BernalPas encore d'évaluation
- Procedure Right Onplacental ExaminationDocument3 pagesProcedure Right Onplacental ExaminationPriyanka SheoranPas encore d'évaluation
- Abnormal Uterine ActionDocument33 pagesAbnormal Uterine ActionRadwa Ebed100% (1)
- CervicitisDocument7 pagesCervicitisElaisa Mae Delos SantosPas encore d'évaluation
- Preparation of Labor RoomDocument3 pagesPreparation of Labor RoomKumar SuryavanshiPas encore d'évaluation
- Health Problems MyselfDocument54 pagesHealth Problems MyselfKrishnaveni Murugesh100% (2)
- Seminor Topic AbortionDocument13 pagesSeminor Topic AbortionBHUKYA USHARANIPas encore d'évaluation
- MeningitisDocument12 pagesMeningitisFaith Vaughn100% (2)
- Care of The Pregnant Woman With HIVDocument34 pagesCare of The Pregnant Woman With HIVJenelle Melinda TullochPas encore d'évaluation
- Diagnosis of PregnancyDocument16 pagesDiagnosis of PregnancySùjâl PätídàrPas encore d'évaluation
- Obg Procedures FinalDocument60 pagesObg Procedures FinalVeena DalmeidaPas encore d'évaluation
- Displacement of The UterusDocument32 pagesDisplacement of The UterusRaja100% (1)
- Induction and Augmentation of LaborDocument20 pagesInduction and Augmentation of Laborjssamc prasootitantraPas encore d'évaluation
- Antenatal CareDocument82 pagesAntenatal Caremdasad18Pas encore d'évaluation
- Disease Condition:: Hyperemsis Gravidarum: DefinitionDocument4 pagesDisease Condition:: Hyperemsis Gravidarum: DefinitionPriyanka JohnPas encore d'évaluation
- The Abnormal PuerperiumDocument25 pagesThe Abnormal PuerperiumMartijn JohanPas encore d'évaluation
- Hiv and Aids in ChildrenDocument36 pagesHiv and Aids in ChildrenKazau FwalangaPas encore d'évaluation
- NEONATAL APNOEA SMNRDocument18 pagesNEONATAL APNOEA SMNRAswathy RC100% (1)
- P PyrexiaDocument23 pagesP PyrexiaRex BishopPas encore d'évaluation
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document7 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDPas encore d'évaluation
- Material On PHYSIOLOGICAL CHANGES DURING PREGNANCYDocument21 pagesMaterial On PHYSIOLOGICAL CHANGES DURING PREGNANCYAnuradha MauryaPas encore d'évaluation
- Congenital AbnormalitiesDocument45 pagesCongenital AbnormalitiesSaad AbdullahPas encore d'évaluation
- E Maternal Adaptations To PregnancyDocument27 pagesE Maternal Adaptations To PregnancyGeraldine PatayanPas encore d'évaluation
- Abnormal Labor PatternDocument85 pagesAbnormal Labor PatternYibelu BazezewPas encore d'évaluation
- Antepartum HemorrhageDocument5 pagesAntepartum Hemorrhagecode-24Pas encore d'évaluation
- Amniotic Fluid EmbolismDocument5 pagesAmniotic Fluid EmbolismPatel AmeePas encore d'évaluation
- EclampsiaDocument41 pagesEclampsiaNyshan KarkiPas encore d'évaluation
- Child With Blood DisorderDocument126 pagesChild With Blood DisorderSivabarathyPas encore d'évaluation
- Presentation1 Cervical BiopsyDocument14 pagesPresentation1 Cervical BiopsyChanta MaharjanPas encore d'évaluation
- HIV in Mothers and ChildrenDocument90 pagesHIV in Mothers and Childrenabubaker100% (1)
- Breast FeedingDocument3 pagesBreast FeedingArla Donissa-Donique Castillon AlviorPas encore d'évaluation
- HydramniosDocument31 pagesHydramniosSpandana DepuruPas encore d'évaluation
- Antepartum Haemorrhage: Women's & Children's ServicesDocument4 pagesAntepartum Haemorrhage: Women's & Children's ServicesYwagar YwagarPas encore d'évaluation
- Maternal and Child Health CareDocument12 pagesMaternal and Child Health CarePraachii SharmaPas encore d'évaluation
- Gynecological Operation and Nursing ManagementDocument29 pagesGynecological Operation and Nursing Managementhawra alsaadPas encore d'évaluation
- Obstetric & Gynecology Nursing: Topic-Physiological Changes During LabourDocument54 pagesObstetric & Gynecology Nursing: Topic-Physiological Changes During LabourBhumi ChouhanPas encore d'évaluation
- Breech PresentationDocument85 pagesBreech Presentationwidya vannesaPas encore d'évaluation
- Color HandoutsDocument23 pagesColor HandoutsAndreea SlabuPas encore d'évaluation
- Chnn211 Lec (Philippine Health Care Delivery System) : The PhilippinesDocument6 pagesChnn211 Lec (Philippine Health Care Delivery System) : The Philippineskristelaaa guevarraPas encore d'évaluation
- ALSO Intrapartum Fetal SurveillanceDocument42 pagesALSO Intrapartum Fetal SurveillanceMc WarsamePas encore d'évaluation
- 4 Steps: Instrument PassingDocument3 pages4 Steps: Instrument PassingGwyn Leen CagasPas encore d'évaluation
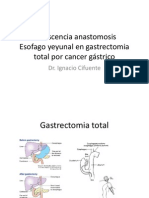
- Dehiscencia Anastomosis Esofago Yeyunal en Gastrectomia Total Por Cancer GástricoDocument22 pagesDehiscencia Anastomosis Esofago Yeyunal en Gastrectomia Total Por Cancer GástriconachooooooooPas encore d'évaluation
- AIA Medical Card - Benefit SummaryDocument1 pageAIA Medical Card - Benefit SummaryLimKangPas encore d'évaluation
- Provisional Restorations: Wael Al-Omari. BDS, Mdentsci, PHDDocument27 pagesProvisional Restorations: Wael Al-Omari. BDS, Mdentsci, PHDMohamed VandettaPas encore d'évaluation
- Placenta PreviaDocument5 pagesPlacenta Previajake_supremoPas encore d'évaluation
- Dopamine vs. Dobutamine: Dopamine or Dobutamine. Prior To Anesthesia, If ImpairedDocument2 pagesDopamine vs. Dobutamine: Dopamine or Dobutamine. Prior To Anesthesia, If ImpairedBilly PeterPas encore d'évaluation
- Ohmeda Modulus II Plus Anesthesia Machine - Service and User ManualDocument213 pagesOhmeda Modulus II Plus Anesthesia Machine - Service and User ManualRoger86% (7)
- Anexa 1A IMM UltraDocument15 pagesAnexa 1A IMM UltraGabriela Diana MedlinePas encore d'évaluation
- Quality Survey QuestionnaireDocument13 pagesQuality Survey QuestionnaireDeepak KaushikPas encore d'évaluation
- Abigail Seidman TestimonyDocument7 pagesAbigail Seidman TestimonySpiritus_FilmsPas encore d'évaluation
- Asphyxia NeonatorumDocument35 pagesAsphyxia NeonatorumMuhammad RagilPas encore d'évaluation
- Toxic Pathologic 2Document19 pagesToxic Pathologic 2Anonymous Xmb6QQvRPas encore d'évaluation
- Maternity Benefits Requirements DocsDocument2 pagesMaternity Benefits Requirements DocsGladys April CatarojaPas encore d'évaluation
- Genitals and Inguinal Assessment-FemaleDocument19 pagesGenitals and Inguinal Assessment-Femalemalyn1218Pas encore d'évaluation
- CV EnglishDocument2 pagesCV EnglishDAMIANPas encore d'évaluation
- My Resume...Document5 pagesMy Resume...Kat TangonanPas encore d'évaluation
- E HEALTH SeminarDocument17 pagesE HEALTH SeminarDev jibreenPas encore d'évaluation
- PasdfDocument8 pagesPasdfHuy LePas encore d'évaluation
- From TH 1) Epartmenl of Pathology, University of Pennsylvania Medical School, 2 Hiladdphia.Document15 pagesFrom TH 1) Epartmenl of Pathology, University of Pennsylvania Medical School, 2 Hiladdphia.Mihai StoicaPas encore d'évaluation
- DafpusDocument3 pagesDafpusOtty Mitha OctrizaPas encore d'évaluation
- Words of Wisdom From and To PhlebotomistsDocument7 pagesWords of Wisdom From and To PhlebotomistsDanhil RamosPas encore d'évaluation
- The Uses and Limitations of The Fetal Biophysical Profile.Document18 pagesThe Uses and Limitations of The Fetal Biophysical Profile.Diego Ortecho100% (1)
- Dentistry Semester 1 SAQDocument4 pagesDentistry Semester 1 SAQKan Chang YuPas encore d'évaluation
- A Nurse-Led Initiative To Improve Patient Safety RRTDocument1 pageA Nurse-Led Initiative To Improve Patient Safety RRTValentina LajqiPas encore d'évaluation