Vous aimerez peut-être aussi
- CASE STUDY Intestinal ObstructionDocument68 pagesCASE STUDY Intestinal ObstructionMaria Paula Bungay91% (22)
- Snell Abdomen Questions AnswersDocument10 pagesSnell Abdomen Questions AnswersBen67% (9)
- Clinical Embryology Leeds AdsDocument1 pageClinical Embryology Leeds AdsWael BadranPas encore d'évaluation
- Embryology of Digestive System1Document62 pagesEmbryology of Digestive System1Gina AnnisahPas encore d'évaluation
- Manual Paper I FinalDocument199 pagesManual Paper I Finalankit pandey100% (1)
- Chemistry Notes MeritnationDocument77 pagesChemistry Notes Meritnationanup20jan100% (1)
- Histology SummaryDocument24 pagesHistology SummaryaelsehamyPas encore d'évaluation
- Case 5 - Embryology of AppendixDocument3 pagesCase 5 - Embryology of Appendixshilviadevi100% (1)
- Dr. Archana Rani Associate Professor Department of Anatomy KGMU UP, LucknowDocument44 pagesDr. Archana Rani Associate Professor Department of Anatomy KGMU UP, LucknowlailaPas encore d'évaluation
- 1 Introduction To The Gastrointestinal SystemDocument7 pages1 Introduction To The Gastrointestinal SystemLinh Phan100% (1)
- Epithelial TissueDocument10 pagesEpithelial Tissuememe bolongonPas encore d'évaluation
- Development of Branchial ArchesDocument4 pagesDevelopment of Branchial ArchesFidz LiankoPas encore d'évaluation
- Introduction To Histology: Preparation of Tissue For Histology Dr. OkoloDocument38 pagesIntroduction To Histology: Preparation of Tissue For Histology Dr. OkoloAbiola NerdPas encore d'évaluation
- Anatomy of the Female BreastDocument18 pagesAnatomy of the Female Breasthabtsh habshaPas encore d'évaluation
- Bone Tissues 1Document38 pagesBone Tissues 1ms_pianist100% (1)
- Respiratory System: StructureDocument29 pagesRespiratory System: StructureDr. Abir Ishtiaq100% (1)
- Chick NeurulationDocument14 pagesChick NeurulationSophia RubiaPas encore d'évaluation
- Liver Functions Guide: Bile, Blood Filtration & MetabolismDocument60 pagesLiver Functions Guide: Bile, Blood Filtration & MetabolismqueenuagPas encore d'évaluation
- Sperm Morphology - 2019 FinalDocument44 pagesSperm Morphology - 2019 FinalDr Jitu moni DasPas encore d'évaluation
- Female Reproductive HistologyDocument59 pagesFemale Reproductive HistologyIta Indriani100% (2)
- Embryology of Urinary SystemDocument4 pagesEmbryology of Urinary SystemZllison Mae Teodoro MangabatPas encore d'évaluation
- Enzymes and Their Importance in Plants and AnimalsDocument4 pagesEnzymes and Their Importance in Plants and Animalsanili50% (2)
- BIOLAB FROG Organ HistologyDocument7 pagesBIOLAB FROG Organ HistologyCloie Anne Rabinetas100% (1)
- Intrdoduction Gis 2 (Associated Organs) : Maya Tejasari Histology DepartmentDocument24 pagesIntrdoduction Gis 2 (Associated Organs) : Maya Tejasari Histology DepartmentIpan YustiartaPas encore d'évaluation
- Pancreas Structure and FunctionsDocument11 pagesPancreas Structure and FunctionsCheng XinvennPas encore d'évaluation
- Anatomy and Physiology - Kidney - ForDocument3 pagesAnatomy and Physiology - Kidney - ForKristelle ModalesPas encore d'évaluation
- Embryology of Urogenital SystemDocument42 pagesEmbryology of Urogenital SystemAngetile Kasanga100% (1)
- Introduction of Anatomy PDFDocument34 pagesIntroduction of Anatomy PDFUohna MoienPas encore d'évaluation
- Embryonic Period: Dr. Khin Ma MADocument34 pagesEmbryonic Period: Dr. Khin Ma MAIbrahim FoondunPas encore d'évaluation
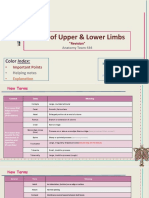
- Bones of Upper and Lower Limbs - RevisionDocument15 pagesBones of Upper and Lower Limbs - RevisionChess Nuts100% (1)
- Early Embryonic DevelopmentDocument19 pagesEarly Embryonic DevelopmentderhangkerPas encore d'évaluation
- The Structure, Function and Organisation of The Human BodyDocument28 pagesThe Structure, Function and Organisation of The Human BodyGemma WhitehousePas encore d'évaluation
- Anatomy of the Hepatobiliary SystemDocument29 pagesAnatomy of the Hepatobiliary SystemKevin KusumanPas encore d'évaluation
- 4 MyologyDocument57 pages4 MyologyAbhijith S. PPas encore d'évaluation
- Histology Exam IV Review Part 2Document26 pagesHistology Exam IV Review Part 2ashdmb217Pas encore d'évaluation
- Anatomy and Physiology: Allen Octaviano Cudiamat, RNDocument29 pagesAnatomy and Physiology: Allen Octaviano Cudiamat, RNᜀᜎ᜔ᜎᜒᜈ᜔ ᜃᜓᜇᜒᜀᜋᜆ᜔Pas encore d'évaluation
- Human Excretory System Removes WasteDocument15 pagesHuman Excretory System Removes WasteJames AysonPas encore d'évaluation
- On Biological Science of Mark Mina and Krichelle Jane LopezDocument5 pagesOn Biological Science of Mark Mina and Krichelle Jane LopezMark MinaPas encore d'évaluation
- Mammary Gland Structure and DevelopmentDocument22 pagesMammary Gland Structure and DevelopmentAaronMaroonFivePas encore d'évaluation
- Histology Practical Manual Part 1 2021Document124 pagesHistology Practical Manual Part 1 2021khushikumari1407Pas encore d'évaluation
- Kidney Anatomy and Histology ExplainedDocument7 pagesKidney Anatomy and Histology ExplainedLaura TorpeyPas encore d'évaluation
- CH - 3 Physics Motion in A Straight LineDocument12 pagesCH - 3 Physics Motion in A Straight LineVENKATESH CHAKRABORTYPas encore d'évaluation
- Biochemistry of Blood Elements: The Figure Is Found at (March 2007)Document37 pagesBiochemistry of Blood Elements: The Figure Is Found at (March 2007)Sadam_fasterPas encore d'évaluation
- AnatomyDocument74 pagesAnatomyhafeez khanPas encore d'évaluation
- Thursday, April 09, 2009 4:45 PMDocument266 pagesThursday, April 09, 2009 4:45 PMkcs2012Pas encore d'évaluation
- Liver and Biliary System: DR Anil Chaudhary Associate Professor PhysiologyDocument31 pagesLiver and Biliary System: DR Anil Chaudhary Associate Professor Physiologylion2chPas encore d'évaluation
- Applied Anatomy and Physiology of the LiverDocument45 pagesApplied Anatomy and Physiology of the Liverpukler1Pas encore d'évaluation
- Anatomy and Physiology Lecture - Midterm (Labelling)Document15 pagesAnatomy and Physiology Lecture - Midterm (Labelling)KRISTINE ZAINAB PUENTEPas encore d'évaluation
- Femoral Region, Anterior and Medial Compartments of The ThighDocument49 pagesFemoral Region, Anterior and Medial Compartments of The ThighNolanPas encore d'évaluation
- Metamorphosis in InsectsDocument13 pagesMetamorphosis in InsectsAnupam GhoshPas encore d'évaluation
- Anatomy and Physiology of Digestive SystemDocument34 pagesAnatomy and Physiology of Digestive SystemIan IsidroPas encore d'évaluation
- 9 Skeletal SystemDocument63 pages9 Skeletal Systemvanderphys100% (1)
- The Gut Tube and Body CavitiesDocument31 pagesThe Gut Tube and Body CavitiesGeoffreyPas encore d'évaluation
- Urogenital SystemDocument5 pagesUrogenital Systemstudent10100Pas encore d'évaluation
- 01 - Embryology (Theory)Document54 pages01 - Embryology (Theory)Simran KashyapPas encore d'évaluation
- ANATOMY: Pelvic 2Document16 pagesANATOMY: Pelvic 2Nur Liyana MohamadPas encore d'évaluation
- MEN1 PPDocument15 pagesMEN1 PPAaron D. PhoenixPas encore d'évaluation
- Lecture 23 - The Urinary SystemDocument46 pagesLecture 23 - The Urinary SystemIhab MoustafaPas encore d'évaluation
- The Cockroach (Periplaneta Americana, L.): An Introduction to Entomology for Students of Science and MedicineD'EverandThe Cockroach (Periplaneta Americana, L.): An Introduction to Entomology for Students of Science and MedicineÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)
- Blood Vessels and Lymphatics in Organ SystemsD'EverandBlood Vessels and Lymphatics in Organ SystemsDavid AbramsonPas encore d'évaluation
- The Paris System For Reporting Urinary CytologyDocument66 pagesThe Paris System For Reporting Urinary CytologyRawa MuhsinPas encore d'évaluation
- Dosing of Common Drugs For Infants and ChildrenDocument2 pagesDosing of Common Drugs For Infants and ChildrenRawa MuhsinPas encore d'évaluation
- Extraskeletal Ewing SarcomaDocument44 pagesExtraskeletal Ewing SarcomaRawa MuhsinPas encore d'évaluation
- Syrup Prescription in Infants and ChildrenDocument1 pageSyrup Prescription in Infants and ChildrenRawa MuhsinPas encore d'évaluation
- Thymoma: Rawa MuhsinDocument53 pagesThymoma: Rawa MuhsinRawa MuhsinPas encore d'évaluation
- Disorders of White Cells and Lymph Nodes - Summary ChartDocument2 pagesDisorders of White Cells and Lymph Nodes - Summary ChartRawa MuhsinPas encore d'évaluation
- Solid Pseudopapillary NeoplasmDocument28 pagesSolid Pseudopapillary NeoplasmRawa MuhsinPas encore d'évaluation
- Hyperacute Rejection of Renal TransplantsDocument26 pagesHyperacute Rejection of Renal TransplantsRawa MuhsinPas encore d'évaluation
- Vascular Disorders - Summary ChartDocument2 pagesVascular Disorders - Summary ChartRawa MuhsinPas encore d'évaluation
- Reactive Mesothelial Hyperplasia: Rawa MuhsinDocument38 pagesReactive Mesothelial Hyperplasia: Rawa MuhsinRawa MuhsinPas encore d'évaluation
- Learning and Retaining Information - Spaced Repetition SystemsDocument40 pagesLearning and Retaining Information - Spaced Repetition SystemsRawa MuhsinPas encore d'évaluation
- Types of Milk Formulas and Their UsesDocument58 pagesTypes of Milk Formulas and Their UsesRawa MuhsinPas encore d'évaluation
- History and Physical Examination TemplateDocument3 pagesHistory and Physical Examination TemplateRawa MuhsinPas encore d'évaluation
- Chemical Mediators of Acute Inflammation - PresentationDocument41 pagesChemical Mediators of Acute Inflammation - PresentationRawa MuhsinPas encore d'évaluation
- Anti-HIV Chemotherapy - HandoutDocument19 pagesAnti-HIV Chemotherapy - HandoutRawa MuhsinPas encore d'évaluation
- Chemical Mediators of Acute Inflammation - HandoutDocument24 pagesChemical Mediators of Acute Inflammation - HandoutRawa MuhsinPas encore d'évaluation
- Embryology Course IX - Urogenital SystemDocument55 pagesEmbryology Course IX - Urogenital SystemRawa MuhsinPas encore d'évaluation
- Anti-HIV Chemotherapy - PresentationDocument39 pagesAnti-HIV Chemotherapy - PresentationRawa MuhsinPas encore d'évaluation
- Tale of The MicrobesDocument62 pagesTale of The MicrobesRawa Muhsin100% (1)
- Breast and Ovarian Cancer - HandoutDocument8 pagesBreast and Ovarian Cancer - HandoutRawa MuhsinPas encore d'évaluation
- Breast and Ovarian Cancer - PresentationDocument26 pagesBreast and Ovarian Cancer - PresentationRawa MuhsinPas encore d'évaluation
- Events in Embryology - Grouped by TimeDocument3 pagesEvents in Embryology - Grouped by TimeRawa Muhsin100% (1)
- Embryology Course VI - Cardiovascular SystemDocument49 pagesEmbryology Course VI - Cardiovascular SystemRawa MuhsinPas encore d'évaluation
- A - O-Rrhea: Lack of - FlowDocument37 pagesA - O-Rrhea: Lack of - FlowRawa MuhsinPas encore d'évaluation
- Embryology Course VII - Musculoskeletal System, Pharyngeal ApparatusDocument62 pagesEmbryology Course VII - Musculoskeletal System, Pharyngeal ApparatusRawa MuhsinPas encore d'évaluation
- Embryology Course I - Introduction, Gametogenesis, ImplantationDocument35 pagesEmbryology Course I - Introduction, Gametogenesis, ImplantationRawa MuhsinPas encore d'évaluation
- Embryology Course II - 2nd and 3rd Weeks of DevelopmentDocument22 pagesEmbryology Course II - 2nd and 3rd Weeks of DevelopmentRawa MuhsinPas encore d'évaluation
- Embryology Course V - Body Cavities, Respiratory SystemDocument28 pagesEmbryology Course V - Body Cavities, Respiratory SystemRawa MuhsinPas encore d'évaluation
- 2.1 Acute InflammationDocument70 pages2.1 Acute InflammationRawa Muhsin100% (1)
- SLCC Anatomy CH 26-Digestive System: Study Online atDocument3 pagesSLCC Anatomy CH 26-Digestive System: Study Online atBrendaJooYeePas encore d'évaluation
- Development of the GIT Part 1Document3 pagesDevelopment of the GIT Part 1Zade BawiPas encore d'évaluation
- ABDOMINAL PARACENTESIS PROCEDUREDocument5 pagesABDOMINAL PARACENTESIS PROCEDUREVijith.V.kumar100% (1)
- Medical Terminology and Anatomy For ICD-10 CodingDocument1 pageMedical Terminology and Anatomy For ICD-10 CodingsrdjanPas encore d'évaluation
- UrologyDocument12 pagesUrologyThakoon Tts100% (1)
- AJCC 8thed TNMDocument34 pagesAJCC 8thed TNMPrarthna PatelPas encore d'évaluation
- FCPS Part 1 SyllabusDocument37 pagesFCPS Part 1 SyllabusMd Hasan Imam100% (2)
- Gynae FCPS 1 Guide-1Document24 pagesGynae FCPS 1 Guide-1Lubna MushtaqPas encore d'évaluation
- Digestive System BAYLONDocument12 pagesDigestive System BAYLONElijah Joaquin Payumo BaylonPas encore d'évaluation
- Tugas Ekspertise AbdomenDocument42 pagesTugas Ekspertise AbdomentriaclaresiaPas encore d'évaluation
- Peritonel DialysisDocument8 pagesPeritonel DialysisSudesh TomarPas encore d'évaluation
- M. P. Rodighiero Peritoneal Dialysis - A Clinical Update Contributions To Nephrology S Karger Pub 2006Document367 pagesM. P. Rodighiero Peritoneal Dialysis - A Clinical Update Contributions To Nephrology S Karger Pub 2006Aciobanitei AlexandraPas encore d'évaluation
- Anaphy Practice TestsDocument6 pagesAnaphy Practice TestsHenie Louise HinanayPas encore d'évaluation
- Lyve1 Macrophages of Murine Peritoneal Mesothelium Promote Omentum-Independent Ovarian Tumor GrowthDocument23 pagesLyve1 Macrophages of Murine Peritoneal Mesothelium Promote Omentum-Independent Ovarian Tumor GrowthHellen StalinPas encore d'évaluation
- Acute Abdomen and PeritonitisDocument17 pagesAcute Abdomen and PeritonitisAnisaPratiwiArumningsihPas encore d'évaluation
- PeritonitisDocument14 pagesPeritonitisAyad IdresPas encore d'évaluation
- Anatomy Quizbook PDFDocument92 pagesAnatomy Quizbook PDFLipid Berger67% (3)
- Perforated Peptic Ulcer DictationDocument4 pagesPerforated Peptic Ulcer DictationHassanPas encore d'évaluation
- Abdominal ParacentesisDocument4 pagesAbdominal ParacentesisRashmi C S100% (1)
- Celom and digestive system labDocument134 pagesCelom and digestive system labLisa WolskiPas encore d'évaluation
- Seeleys Anatomy Physiology 10th Edition Test Bank Cinnamon VanputteDocument61 pagesSeeleys Anatomy Physiology 10th Edition Test Bank Cinnamon VanputteHorace Samuel100% (28)
- Abdominal Pain in ChildrenDocument36 pagesAbdominal Pain in ChildrenKiani LarasPas encore d'évaluation
- Peritonitis and Abdominal Sepsis Background, Anatomy, PathophysiologyDocument1 pagePeritonitis and Abdominal Sepsis Background, Anatomy, PathophysiologyFlora Eka HeinzendorfPas encore d'évaluation
- Sectio CaesareaDocument13 pagesSectio CaesareaDavid ZamrilPas encore d'évaluation
- Pelvic Lymphadenectomy Step-By-Step Surgical EducaDocument5 pagesPelvic Lymphadenectomy Step-By-Step Surgical EducaVlad GrigorePas encore d'évaluation
- MRCS B VivaDocument8 pagesMRCS B Vivatahir_the_great2939Pas encore d'évaluation
- General Arrangement of The Abdominal ViserasDocument14 pagesGeneral Arrangement of The Abdominal ViserasShimmering MoonPas encore d'évaluation
- What Is PeritonitisDocument9 pagesWhat Is PeritonitisArsitoPas encore d'évaluation