Vous aimerez peut-être aussi
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Think Before Buying: ReadingDocument1 pageThink Before Buying: ReadingadrianmaiarotaPas encore d'évaluation
- FutbolistaDocument18 pagesFutbolistaKaren Osses50% (2)
- Bioclim MaxentDocument9 pagesBioclim MaxentNicolás FrutosPas encore d'évaluation
- Morality Speaks of A System of Behavior in Regards To Standards of Right or Wrong Behavior. The WordDocument3 pagesMorality Speaks of A System of Behavior in Regards To Standards of Right or Wrong Behavior. The WordTHEO DOMINIC REQUERME SILVOSAPas encore d'évaluation
- Antena Kathrein 742266 PDFDocument2 pagesAntena Kathrein 742266 PDFcesarbayonaPas encore d'évaluation
- Comparison of Ozone Vs Uv in WaterDocument1 pageComparison of Ozone Vs Uv in WaterRajesh PandeyPas encore d'évaluation
- E2870-13 Standard Test Method For Evaluating RelativDocument6 pagesE2870-13 Standard Test Method For Evaluating RelativA MusaverPas encore d'évaluation
- Brochure E-AIR T400-900 WEG APP 2958 1020 02 ENDocument3 pagesBrochure E-AIR T400-900 WEG APP 2958 1020 02 ENDaniel BravoPas encore d'évaluation
- Prepared by (Hospital Pharmacist) Primary & Secondary Healthcare DepartmentDocument11 pagesPrepared by (Hospital Pharmacist) Primary & Secondary Healthcare DepartmentwaqasPas encore d'évaluation
- Furuno FM 8700 Users Manual 429122Document102 pagesFuruno FM 8700 Users Manual 429122Igor MaranguanhePas encore d'évaluation
- The Girl Who CanDocument4 pagesThe Girl Who CanMadhu50% (2)
- Application of Land Suitability AnalysisDocument16 pagesApplication of Land Suitability AnalysisHải Anh Nguyễn100% (1)
- Devi Narayaneeyam - Dasakam 9 Bhuvaneswari Darsanam - Seeing of BhuvaneswariDocument7 pagesDevi Narayaneeyam - Dasakam 9 Bhuvaneswari Darsanam - Seeing of BhuvaneswaribrindaPas encore d'évaluation
- Unipoxy LiningDocument3 pagesUnipoxy LiningDien Thoai Nguyen HuuPas encore d'évaluation
- Chapter Eight - Vapour Compression CycleDocument37 pagesChapter Eight - Vapour Compression Cyclealhusseny100% (1)
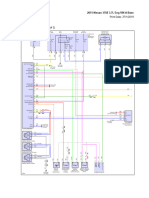
- 2015 Nissan 370Z 3.7L Eng VIN A BaseDocument69 pages2015 Nissan 370Z 3.7L Eng VIN A BaseData TécnicaPas encore d'évaluation
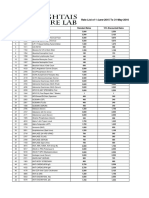
- Rate List of 1-June-2015 To 31-May-2016: S.No Code Test Name Standard Rates 15% Discounted RatesDocument25 pagesRate List of 1-June-2015 To 31-May-2016: S.No Code Test Name Standard Rates 15% Discounted RatesMirza BabarPas encore d'évaluation
- Ycaj CHILLERDocument108 pagesYcaj CHILLERAbhilash Joseph100% (2)
- D20 25 30 33S-5 D35C-5 (Sb1109e06) PDFDocument424 pagesD20 25 30 33S-5 D35C-5 (Sb1109e06) PDFGORD100% (8)
- Clinical Science of Guilen Barren SyndromeDocument2 pagesClinical Science of Guilen Barren SyndromemanakimanakuPas encore d'évaluation
- Eye Examination: Dr. Seng Serey / Prof .Kenn Freedman Prof - Kong PisethDocument78 pagesEye Examination: Dr. Seng Serey / Prof .Kenn Freedman Prof - Kong PisethSela KHPas encore d'évaluation
- Theory-Set & Relations PDFDocument4 pagesTheory-Set & Relations PDFmp SinghPas encore d'évaluation
- C.4. Quiz Conservation of BiodiversityDocument2 pagesC.4. Quiz Conservation of Biodiversitylaura pongutaPas encore d'évaluation
- Board of Technical Education Uttar Pradesh Lucknow: CODE 2298Document2 pagesBoard of Technical Education Uttar Pradesh Lucknow: CODE 2298Md Shaaz100% (1)
- ClassnotesonbasicDC DCconverters EP N4Document23 pagesClassnotesonbasicDC DCconverters EP N4Gerardo Treviño GarciaPas encore d'évaluation
- Catálogo DP InglêsDocument20 pagesCatálogo DP Inglêsjf2003Pas encore d'évaluation
- Proyector SNF 111Document3 pagesProyector SNF 111Liliana Patricia PederneraPas encore d'évaluation
- How To Make FireworksDocument14 pagesHow To Make FireworksLeonardo BiancoPas encore d'évaluation
- Material Control Procedure - TemplateDocument5 pagesMaterial Control Procedure - TemplateHernandito Rahmat KusumaPas encore d'évaluation
- Disorders of The Endocrine System and Dental ManagementDocument63 pagesDisorders of The Endocrine System and Dental ManagementSanni FatimaPas encore d'évaluation