Vous aimerez peut-être aussi
- Systemic MycosesMDocument43 pagesSystemic MycosesMMaxamed Faarax XaashiPas encore d'évaluation
- Chapter 5 Medically Most Important BacteriaDocument5 pagesChapter 5 Medically Most Important BacteriaclarissePas encore d'évaluation
- Abhi 99 % SarifDocument10 pagesAbhi 99 % SarifravinchauhanPas encore d'évaluation
- ACTINOMYCETESDocument22 pagesACTINOMYCETESDaniel WaweruPas encore d'évaluation
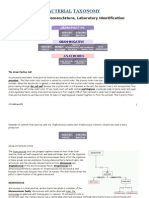
- Bacterial TaxonomyDocument185 pagesBacterial Taxonomyshbv1Pas encore d'évaluation
- Bacteriology Pa Exam Topics: Laboratory Diagnosis in Infections Cause byDocument20 pagesBacteriology Pa Exam Topics: Laboratory Diagnosis in Infections Cause byCristina KepteaPas encore d'évaluation
- AnthraxDocument20 pagesAnthraxBanabas KluPas encore d'évaluation
- Mycology 1 SDocument29 pagesMycology 1 SYassine MeradPas encore d'évaluation
- StreptomycesDocument13 pagesStreptomycesraheemrahi089Pas encore d'évaluation
- Groupone MycologyDocument14 pagesGroupone MycologyTilahun TesemaPas encore d'évaluation
- Actinomicosis: by Ahmed RabieDocument8 pagesActinomicosis: by Ahmed RabieAhmad RabiePas encore d'évaluation
- Free Living Amebae 2020 DR OtionoDocument44 pagesFree Living Amebae 2020 DR OtionoGeoffreyPas encore d'évaluation
- Identification and Classification According To Bergy's Manual of Systemic Bacteriology 2Document46 pagesIdentification and Classification According To Bergy's Manual of Systemic Bacteriology 2Cezar Alexander GuevaraPas encore d'évaluation
- Stachybotrys Species Black MoldDocument20 pagesStachybotrys Species Black MoldImwaniki21Pas encore d'évaluation
- Day 9 Mycology & Applied January 2021Document338 pagesDay 9 Mycology & Applied January 2021ShriefElghazalyPas encore d'évaluation
- Micro L22Document18 pagesMicro L22Abd Al Kareem RashedPas encore d'évaluation
- Subcutaneous Mycosis: DR Sulaiman ContehDocument17 pagesSubcutaneous Mycosis: DR Sulaiman ContehAbubakar JallohPas encore d'évaluation
- ActinomycosisDocument26 pagesActinomycosistummalapalli venkateswara rao100% (1)
- Part-2-ParasitologyDocument33 pagesPart-2-ParasitologyAli AhmedPas encore d'évaluation
- StreptococcusDocument3 pagesStreptococcusAlvin Anique MandacPas encore d'évaluation
- Bacillus and Biological Warfare: Dr. Samah Binte Latif M - Phil (Part-1), Microbiology Dhaka Medical CollegeDocument67 pagesBacillus and Biological Warfare: Dr. Samah Binte Latif M - Phil (Part-1), Microbiology Dhaka Medical CollegeTania.dmp20Pas encore d'évaluation
- Opportunistic MycosisDocument59 pagesOpportunistic MycosisSisay Fesseha AmbayePas encore d'évaluation
- SputumDocument28 pagesSputumfniegas172Pas encore d'évaluation
- Actinomycetes: by Professor Zainab A. AldhaherDocument10 pagesActinomycetes: by Professor Zainab A. Aldhaherمروه عماد عيسىPas encore d'évaluation
- Fungal DiseasesDocument96 pagesFungal DiseasesKhateeja Tul KubraPas encore d'évaluation
- Fungal Mycosis and Other InfectionsDocument34 pagesFungal Mycosis and Other InfectionsRajeev PotadarPas encore d'évaluation
- Fungal Infections of The Lower Respiratory Tract Disease Additional InformationDocument2 pagesFungal Infections of The Lower Respiratory Tract Disease Additional InformationAnnahPas encore d'évaluation
- Short Writing Assignment 4Document5 pagesShort Writing Assignment 4Troi JeraoPas encore d'évaluation
- Faculty of Health Sciences: DepartmentDocument35 pagesFaculty of Health Sciences: DepartmentAbdirashiid Mahdi HirsiPas encore d'évaluation
- Pathogenic and Free Living Amoeba Sikatema MikeDocument33 pagesPathogenic and Free Living Amoeba Sikatema MikebrainworxeducationPas encore d'évaluation
- Actinomyces, Nocardia and Tropheryma: Actinomycosis Nocardiasis Whipple's DiseaseDocument4 pagesActinomyces, Nocardia and Tropheryma: Actinomycosis Nocardiasis Whipple's Diseasenour achkarPas encore d'évaluation
- Grp01ClinPara PDFDocument68 pagesGrp01ClinPara PDFJeddhie MoraPas encore d'évaluation
- Mycology - Chapter Six Dimorphic Fungi: BLASTOMYCOSIS (Blastomyces Dermatitidis)Document16 pagesMycology - Chapter Six Dimorphic Fungi: BLASTOMYCOSIS (Blastomyces Dermatitidis)ginarsih99_hutamiPas encore d'évaluation
- Introduction To Medical MycologyDocument39 pagesIntroduction To Medical Mycologyamael saint-louisPas encore d'évaluation
- 6 InfectionsDocument71 pages6 InfectionsSravani PeddagangannagariPas encore d'évaluation
- Scopulariopsis AcremoniumDocument20 pagesScopulariopsis Acremoniumdpdmello8532Pas encore d'évaluation
- Fungal Infections Mycotic Infections MycosesDocument12 pagesFungal Infections Mycotic Infections MycosesHussein QasimPas encore d'évaluation
- HML 316 Notes 2021Document39 pagesHML 316 Notes 2021nessa nimoPas encore d'évaluation
- Mycology: Fairy Ring MushroomsDocument41 pagesMycology: Fairy Ring MushroomsFarhan Azmain Fahim100% (2)
- Opportunistic Amoebiasis: Causal AgentsDocument144 pagesOpportunistic Amoebiasis: Causal AgentsJOSEPH NDERITUPas encore d'évaluation
- Micp ReviewerDocument30 pagesMicp ReviewerFrancisca NairPas encore d'évaluation
- Systemic MycosisDocument49 pagesSystemic Mycosisማላያላም ማላያላምPas encore d'évaluation
- 1.2 - Bacillus AnthracisDocument26 pages1.2 - Bacillus Anthracissajad abasPas encore d'évaluation
- Tropical Pathology of The Oral MucosaDocument20 pagesTropical Pathology of The Oral MucosaGeorgi GugicevPas encore d'évaluation
- The Pathogen MDSC-1405Document70 pagesThe Pathogen MDSC-1405Ismadth2918388Pas encore d'évaluation
- Dr. Keli Mem203 MycologyDocument46 pagesDr. Keli Mem203 Mycologykaregagladys90Pas encore d'évaluation
- (I2M Week 6-7) Multicellular PathogensDocument40 pages(I2M Week 6-7) Multicellular PathogensellaPas encore d'évaluation
- Schistosomes Parasite in HumanDocument27 pagesSchistosomes Parasite in HumanAnonymous HXLczq3Pas encore d'évaluation
- Fungi & Systemic MycosesDocument49 pagesFungi & Systemic MycosesAmal ShereefPas encore d'évaluation
- Opportunistic Mycoses - Zygomycosis, AspergillosisDocument44 pagesOpportunistic Mycoses - Zygomycosis, Aspergillosisansar ckPas encore d'évaluation
- Lab Animal BacterialDocument28 pagesLab Animal BacterialRakeshPas encore d'évaluation
- 10 - Medical MycologyDocument74 pages10 - Medical Mycologyjames rukenyaPas encore d'évaluation
- Eukaryotic Diseases - 06Document33 pagesEukaryotic Diseases - 06Vien WhitlockPas encore d'évaluation
- Bacteria of Medical Importance 1Document21 pagesBacteria of Medical Importance 1Tshepang MohlahloPas encore d'évaluation
- Non-Pathogenic Amoeba - Free LivingDocument42 pagesNon-Pathogenic Amoeba - Free Livingمحمد رحيم حسن محمودPas encore d'évaluation
- 11 NSF Gram + RodsDocument7 pages11 NSF Gram + RodsASECO LISHPas encore d'évaluation
- Proceedings of the First International Congress of Parasitology: Roma, 21-26 September 1964D'EverandProceedings of the First International Congress of Parasitology: Roma, 21-26 September 1964Augusto CorradettiPas encore d'évaluation
- Immunotoxins and Cancer Therapy: Zheng Li, Tao Yu, Ping Zhao and Jie MaDocument7 pagesImmunotoxins and Cancer Therapy: Zheng Li, Tao Yu, Ping Zhao and Jie Mayota_ahlyPas encore d'évaluation
- 7418 PiDocument2 pages7418 Piyota_ahlyPas encore d'évaluation
- Automated Blood Culture: BactecDocument21 pagesAutomated Blood Culture: Bactecyota_ahlyPas encore d'évaluation
- Urine Specimen CollectionDocument3 pagesUrine Specimen Collectionyota_ahlyPas encore d'évaluation
- JURNAL KedokteranDocument6 pagesJURNAL KedokteranGede Ardi SaputraPas encore d'évaluation
- Treating Double VisionDocument2 pagesTreating Double VisionNi Kadek Sri WidiyantiPas encore d'évaluation
- Common Posture Faults: University of Eastern PhilippinesDocument10 pagesCommon Posture Faults: University of Eastern PhilippinesEdgar ElgortPas encore d'évaluation
- Acls Study GuideDocument24 pagesAcls Study GuideMohammad Gita100% (17)
- Kalkstein Dissertation2005Document76 pagesKalkstein Dissertation2005Petruța MarianPas encore d'évaluation
- Oxygen TherapyDocument6 pagesOxygen Therapy11darnell100% (1)
- Science Investigatory ProjectDocument15 pagesScience Investigatory ProjectHannah Coleen Nacion68% (19)
- Resume BrixDocument2 pagesResume Brixapi-530223646Pas encore d'évaluation
- NCP MyomaDocument6 pagesNCP MyomaIzza Mae Ferrancol PastranaPas encore d'évaluation
- Prof BSP - Neurologic Paraneoplastic SyndromesDocument122 pagesProf BSP - Neurologic Paraneoplastic SyndromesSavitha BasriPas encore d'évaluation
- MudreDocument10 pagesMudrejezebelvertPas encore d'évaluation
- Masi 2003Document21 pagesMasi 2003Stijn VanheulePas encore d'évaluation
- PsmsformsDocument1 pagePsmsformsapi-261670650Pas encore d'évaluation
- Third Molar Surgery and Associated ComplicationsDocument10 pagesThird Molar Surgery and Associated ComplicationsBasil JacobPas encore d'évaluation
- Brexpiprazole: A Review of A New Treatment Option For Schizophrenia and Major Depressive DisorderDocument6 pagesBrexpiprazole: A Review of A New Treatment Option For Schizophrenia and Major Depressive DisorderLuis Pablo HsPas encore d'évaluation
- Kidney & HeartDocument72 pagesKidney & Heartwaftmovers100% (1)
- Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis Management, Prognosis and Long Term SequelaeDocument28 pagesStevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis Management, Prognosis and Long Term SequelaePutri SRPas encore d'évaluation
- Introduction To Medical RoboticsDocument83 pagesIntroduction To Medical RoboticsBogdan OlaruPas encore d'évaluation
- Gallbladder - Gallstones and SurgeryDocument4 pagesGallbladder - Gallstones and SurgeryVinod MeenaPas encore d'évaluation
- The Aetiology of Gingival RecessionDocument4 pagesThe Aetiology of Gingival RecessionshahidibrarPas encore d'évaluation
- Training Program: By: Rahul AhujaDocument17 pagesTraining Program: By: Rahul Ahujakei HoinaPas encore d'évaluation
- Test 5 - QUIZDocument9 pagesTest 5 - QUIZClaudia Lucía Zuñiga Guevara67% (6)
- Professional Portfolio 2007Document2 pagesProfessional Portfolio 2007api-276072200100% (1)
- Bhamashah Swasthya Bima Yojana 2017-19: S. No. Final Package Name Package Type Proposed Rate Speciality Code Short NameDocument21 pagesBhamashah Swasthya Bima Yojana 2017-19: S. No. Final Package Name Package Type Proposed Rate Speciality Code Short Nameswastik hospitalPas encore d'évaluation
- Procrastination Research PaperDocument8 pagesProcrastination Research Paperapi-483126344Pas encore d'évaluation
- Homeopatie RomaniaDocument11 pagesHomeopatie RomaniaAnaPas encore d'évaluation
- Khan, Chap 11Document63 pagesKhan, Chap 11E. Saeedzadeh100% (1)
- Controlled Release Oral Drug Delivery SystemsDocument37 pagesControlled Release Oral Drug Delivery Systemsamitchauhan09Pas encore d'évaluation
- Occupational Therapy Interventions For ADHD - A Systematic ReviewDocument71 pagesOccupational Therapy Interventions For ADHD - A Systematic ReviewAkshayaaPas encore d'évaluation
- Nursing Health Assessment MnemonicsDocument20 pagesNursing Health Assessment Mnemonicsmildred alidonPas encore d'évaluation