Vous aimerez peut-être aussi
- Leptospirosis: Dr. Doni Priambodo Wijisaksono, Sppd-KptiDocument33 pagesLeptospirosis: Dr. Doni Priambodo Wijisaksono, Sppd-KptialbaazaPas encore d'évaluation
- DRG - Ivan Arie Wahyudi, M. Kes., PH.DDocument28 pagesDRG - Ivan Arie Wahyudi, M. Kes., PH.DMaudina PamelaPas encore d'évaluation
- DengueDocument65 pagesDengueShajahan SideequePas encore d'évaluation
- Lepto Fkumi 2021Document43 pagesLepto Fkumi 2021Asbar Fatur MuhPas encore d'évaluation
- Causes of Drowsiness in This PatientDocument12 pagesCauses of Drowsiness in This PatientNu JoePas encore d'évaluation
- Denguefinalpdf-170803082145 2Document74 pagesDenguefinalpdf-170803082145 2L. HusnaPas encore d'évaluation
- Leptospirosis: Nurul Hidayu - Nashriq Aiman - Audi AdibahDocument28 pagesLeptospirosis: Nurul Hidayu - Nashriq Aiman - Audi AdibahAkshay D'souzaPas encore d'évaluation
- Division of Infectious and Tropical Diseases, Department of Internal Medicine, University of Sumatera Utara/ Adam Malik Hospital, Medan, IndonesiaDocument18 pagesDivision of Infectious and Tropical Diseases, Department of Internal Medicine, University of Sumatera Utara/ Adam Malik Hospital, Medan, IndonesiaIndah PutriPas encore d'évaluation
- Rickettsial InfectionsDocument45 pagesRickettsial InfectionsTarikPas encore d'évaluation
- Lymph Ad en Op A ThyDocument24 pagesLymph Ad en Op A ThyAlyaa El SayedPas encore d'évaluation
- Communicable Diseases: Roberto M. Salvador Jr. R.N.,M.D. Infectious and Tropical Disease SpecialistDocument846 pagesCommunicable Diseases: Roberto M. Salvador Jr. R.N.,M.D. Infectious and Tropical Disease SpecialistGrn Mynjrkxz100% (1)
- Leptospirosis UPH 2Document33 pagesLeptospirosis UPH 2Joshua ObrienPas encore d'évaluation
- Infectious DiseasesDocument140 pagesInfectious DiseasesSamah IzzPas encore d'évaluation
- Salmonella InfectionsDocument3 pagesSalmonella InfectionsYolanda Dwi OktaviyaniPas encore d'évaluation
- The Common Cases of Infectious Disease: An Approach To DiagnosisDocument29 pagesThe Common Cases of Infectious Disease: An Approach To DiagnosisAlizaPinkyPas encore d'évaluation
- Leptospirosis in Dr. Soetomo SBYDocument18 pagesLeptospirosis in Dr. Soetomo SBYanwar1hidayatPas encore d'évaluation
- Journal Reading PersentationDocument31 pagesJournal Reading PersentationKartikaEkaWulandariPas encore d'évaluation
- Leptospirosis: Dr. Doni Priambodo Wijisaksono Sppd-KptiDocument33 pagesLeptospirosis: Dr. Doni Priambodo Wijisaksono Sppd-KptiFarika NorPas encore d'évaluation
- S Infective EndocarditisDocument24 pagesS Infective EndocarditisMpanso Ahmad AlhijjPas encore d'évaluation
- LEPTOSPIROSIS Power Point PresDocument22 pagesLEPTOSPIROSIS Power Point PresAlex Guevarra100% (1)
- 8.3 Medicine - Tropical Infectious Diseases Leptospirosis 2014ADocument7 pages8.3 Medicine - Tropical Infectious Diseases Leptospirosis 2014ABhi-An BatobalonosPas encore d'évaluation
- Kawasaki DiseaseDocument41 pagesKawasaki DiseaseWuryan Dewi Mftahtyas ArumPas encore d'évaluation
- Leptospirosis, Typhoid and Other FeversDocument37 pagesLeptospirosis, Typhoid and Other FeverskarageePas encore d'évaluation
- Case of LeptospirosisDocument60 pagesCase of LeptospirosisNoreen Cala-MayubayPas encore d'évaluation
- Dengue Fever 2Document21 pagesDengue Fever 2dr9348345000Pas encore d'évaluation
- 05 - Sle, DMZ, PHSDocument157 pages05 - Sle, DMZ, PHSG SPas encore d'évaluation
- LeptospirosisDocument10 pagesLeptospirosisrommel f irabagonPas encore d'évaluation
- Lecture Infective EndocarditisDocument37 pagesLecture Infective EndocarditisJohnson OlawalePas encore d'évaluation
- Superficial Infection and SepisDocument35 pagesSuperficial Infection and Sepissanjivdas100% (1)
- LeptospirosisDocument7 pagesLeptospirosisFarah Nadia MoksinPas encore d'évaluation
- IM Infective Endocarditis Pericardial DiseaseDocument4 pagesIM Infective Endocarditis Pericardial DiseaseLucyellowOttemoesoePas encore d'évaluation
- Systemic Lupus Erythematosus: Harrison's ClubDocument60 pagesSystemic Lupus Erythematosus: Harrison's ClubOrchid Limoso LozanoPas encore d'évaluation
- AudioDocument50 pagesAudioshortysdavidPas encore d'évaluation
- Systemic Lupus Erythematosus - An Overview: - Dr. Parvez KhanDocument68 pagesSystemic Lupus Erythematosus - An Overview: - Dr. Parvez KhanMohammad Sadiq AzamPas encore d'évaluation
- NCM118 ReportDocument35 pagesNCM118 ReportJoy Ce VeralloPas encore d'évaluation
- Dengue: (Mosquito Borne)Document45 pagesDengue: (Mosquito Borne)Sibi PalanisamyPas encore d'évaluation
- Asculitis Syndromes: Emily B. Martin, MD Rheumatology Board Review April 9, 2008Document54 pagesAsculitis Syndromes: Emily B. Martin, MD Rheumatology Board Review April 9, 2008Miguel M. Melchor RodríguezPas encore d'évaluation
- Joel Vasanth PeterDocument38 pagesJoel Vasanth PeterJoelPeterPas encore d'évaluation
- Referat SepsisDocument18 pagesReferat SepsisImelva GirsangPas encore d'évaluation
- LeptospirosisDocument9 pagesLeptospirosisDeepu VijayaBhanuPas encore d'évaluation
- SleDocument33 pagesSleZaira HussainPas encore d'évaluation
- Fever With Jaundice and A Purpuric RashDocument4 pagesFever With Jaundice and A Purpuric RashRaida Uceda GarniquePas encore d'évaluation
- Sigal Immuno DeficiencyDocument61 pagesSigal Immuno DeficiencyClaire HendersonPas encore d'évaluation
- Malaria and LeptospirosisDocument18 pagesMalaria and LeptospirosisRasYa DIPas encore d'évaluation
- Leukocytic Disorders: Non-Neoplastic AlterationsDocument36 pagesLeukocytic Disorders: Non-Neoplastic AlterationsIseth ISethPas encore d'évaluation
- Infective EndocarditisDocument12 pagesInfective EndocarditisYoulin KohPas encore d'évaluation
- Lepto Spiros IsDocument7 pagesLepto Spiros IslansoprazolePas encore d'évaluation
- Infective EndocarditisDocument57 pagesInfective EndocarditisRika FitriaPas encore d'évaluation
- Fever Online SessionDocument51 pagesFever Online SessionPrecious ChaiPas encore d'évaluation
- Leptospirosis in ChildrenDocument5 pagesLeptospirosis in ChildrenPramod KumarPas encore d'évaluation
- Gil P. Soriano, RN, MhpedDocument24 pagesGil P. Soriano, RN, MhpedGil Platon SorianoPas encore d'évaluation
- Fortfolio of ARIFDocument20 pagesFortfolio of ARIFWaqas AhmadPas encore d'évaluation
- Dengue Feve1Document10 pagesDengue Feve1Santhosh KumarPas encore d'évaluation
- Nephrotic SyndromeDocument24 pagesNephrotic SyndromeSamah KhanPas encore d'évaluation
- Leptospirosis: Causes, Incidence, and Risk FactorsDocument6 pagesLeptospirosis: Causes, Incidence, and Risk FactorsJackii DoronilaPas encore d'évaluation
- The Diagnosis and Management of CellulitisDocument20 pagesThe Diagnosis and Management of Cellulitisomkar.rakomPas encore d'évaluation
- Referat SLEDocument24 pagesReferat SLENihayatulHusniaPas encore d'évaluation
- Dengue-Who Treatment ProtocolsDocument39 pagesDengue-Who Treatment ProtocolsushapadminivadivelswamyPas encore d'évaluation
- Bio MalariaDocument10 pagesBio MalariaAnonymous 42shXQPSjPas encore d'évaluation
- What Is Benign Prostatic HyperplasiaDocument3 pagesWhat Is Benign Prostatic HyperplasiaLeo CortinaPas encore d'évaluation
- Thomas Jonnesco - Remarks On General Spinal Analgesia (1909) .Document6 pagesThomas Jonnesco - Remarks On General Spinal Analgesia (1909) .BigBoss_GRUPas encore d'évaluation
- Diabetes & Metabolic Syndrome: Clinical Research & Reviews: Ganiyu Oboh, Ayokunle O. AdemosunDocument5 pagesDiabetes & Metabolic Syndrome: Clinical Research & Reviews: Ganiyu Oboh, Ayokunle O. AdemosunDian Ayu ChotimahPas encore d'évaluation
- Critical Periods in A Puppy LifeDocument7 pagesCritical Periods in A Puppy Lifeapi-208346542Pas encore d'évaluation
- RPD M C Q With AnswersDocument23 pagesRPD M C Q With Answersيارا حسين81% (16)
- Anterior RhinosDocument4 pagesAnterior RhinosYohan YudhantoPas encore d'évaluation
- Medisinsk Rapport Ørebetennelse Ole Fjeld HaugstvedtDocument2 pagesMedisinsk Rapport Ørebetennelse Ole Fjeld HaugstvedtOle HaugstvedtPas encore d'évaluation
- In Search of The Later HahhemannDocument9 pagesIn Search of The Later HahhemannJuan Jose JuarezPas encore d'évaluation
- Essential Intrapartum and Newborn CareDocument2 pagesEssential Intrapartum and Newborn CareNikka Moreen DagdagPas encore d'évaluation
- Ayurvedic Management of Dysfunctional Uterine Bleeding A Case StudyDocument3 pagesAyurvedic Management of Dysfunctional Uterine Bleeding A Case StudyTarun PandianPas encore d'évaluation
- Reference Values in Veterinary MedicineDocument4 pagesReference Values in Veterinary MedicineSam VargesePas encore d'évaluation
- Physical Form 2018Document2 pagesPhysical Form 2018api-247134277Pas encore d'évaluation
- WELVET701EN - GLUCO CALEA - FolderDocument20 pagesWELVET701EN - GLUCO CALEA - FolderandreisandorPas encore d'évaluation
- Carestart TM MalariaDocument3 pagesCarestart TM MalariaQaiser ZamanPas encore d'évaluation
- ECG Interpretation BookDocument57 pagesECG Interpretation BookLouis Plan100% (2)
- Nauli - Abdominal MassageDocument3 pagesNauli - Abdominal Massagedd1242000Pas encore d'évaluation
- Correlative AnatomyDocument19 pagesCorrelative AnatomyLicensed to HealPas encore d'évaluation
- Ionus Compendium of Strange CreaturesDocument74 pagesIonus Compendium of Strange CreaturesAndrey Augusto100% (3)
- Desai 2013Document3 pagesDesai 2013Indah PratiwiPas encore d'évaluation
- Intermediate Biology Olympiad SyllabusDocument2 pagesIntermediate Biology Olympiad SyllabuspPas encore d'évaluation
- Normal Anatomy, Histology, and Spontaneous Pathology of The Nasal Cavity of The Cynomolgus Monkey (Macaca Fascicularis)Document19 pagesNormal Anatomy, Histology, and Spontaneous Pathology of The Nasal Cavity of The Cynomolgus Monkey (Macaca Fascicularis)Dina SartikaPas encore d'évaluation
- Dengue Prevention and Control ProgramDocument7 pagesDengue Prevention and Control Programhazel mirandaPas encore d'évaluation
- NCP-Ineffective Airway ClearanceDocument13 pagesNCP-Ineffective Airway ClearancePaulo Manlangit86% (22)
- Prepared By: Dr. Ma. Angelita S. Rabanal, RN, MSNDocument9 pagesPrepared By: Dr. Ma. Angelita S. Rabanal, RN, MSNAngie SaquingPas encore d'évaluation
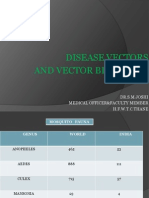
- Disease Vectors and Vector BionomicsDocument16 pagesDisease Vectors and Vector BionomicsSuhas JoshiPas encore d'évaluation
- Tisu Neural Neurofisiologi Neuron Neuroglia Terminologi SarafDocument141 pagesTisu Neural Neurofisiologi Neuron Neuroglia Terminologi SarafRainne LeePas encore d'évaluation
- 144 DiagnosaDocument16 pages144 Diagnosagek yoshiPas encore d'évaluation
- Postnatal Growth and Development: Yenny Yustisia Dept. of Oral Biology Dentistry UNEJDocument38 pagesPostnatal Growth and Development: Yenny Yustisia Dept. of Oral Biology Dentistry UNEJMelisa Novitasari100% (1)
- 2 - Regional Anatomy (MidTerm) MCQsDocument18 pages2 - Regional Anatomy (MidTerm) MCQsManju ShreePas encore d'évaluation