Académique Documents
Professionnel Documents
Culture Documents
Obstetrics 5-1
Transféré par
Dwi cahyaniTitre original
Copyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Obstetrics 5-1
Transféré par
Dwi cahyaniDroits d'auteur :
Formats disponibles
OBSTETRICS
Perinatal Outcomes of Twin Anemia–
Polycythemia Sequence: A Systematic Review
A. Cristina Rossi, MD,1 Federico Prefumo, MD, PhD2
Department of Obstetrics and Gynecology, University of Bari, Bari, Italy
1
Maternal-Fetal Medicine Unit, Department of Obstetrics and Gynecology, University of Brescia, Brescia, Italy
2
Abstract Résumé
Objective: To analyze outcomes of monochorionic twins with twin Objectif : Analyser les issues que connaissent les jumeaux monozygotes
anemia-polycythemia sequence (TAPS). qui présentent une séquence anémie-polyglobulie gémellaire
(twin anemia-polycythemia sequence ou TAPS).
Data Sources: PubMed, EMBASE, Medline, and reference list.
Sources de données : PubMed, EMBASE, Medline et liste de références.
Study Selection: We included reports of TAPS defined prenatally with
abnormal Doppler studies of middle cerebral artery and normal Sélection des études : Nous avons inclus les études ayant porté sur la
amniotic fluid volume which reported data as proportional rates. TAPS établie avant la naissance (obtention de résultats anormaux aux
études Doppler visant l’artère cérébrale moyenne et constatation d’un
Data Extraction: Abstracted outcomes were postnatal hemoglobin
volume normal de liquide amniotique) qui signalaient leurs données
levels, postnatal procedures, and survival rates. Outcomes were
sous forme de taux proportionnels.
analyzed for gestational age at diagnosis of TAPS (15 to 23 weeks,
24 to 29 weeks, > 29 weeks), in utero therapy, and nature of onset Extraction des données : Les issues résumées ont été les suivantes :
(isolated TAPS, or following twin-to-twin transfusion syndrome). The taux postnataux d’hémoglobine, interventions postnatales et taux de
review was performed using MOOSE guidelines. Differences were survie. Les issues ont été analysées en fonction de l’âge gestationnel
significant if P < 0.05. au moment du diagnostic de TAPS (15-23 semaines, 24-29 semaines,
> 29 semaines), de la présence d’un traitement in utero et de la nature
Data Synthesis: We assessed data on 28 pregnancies with TAPS.
de l’apparition de la TAPS (TAPS isolée ou apparaissant à la suite du
Diagnosis at 15 to 23 weeks’ gestation and in utero therapy
syndrome transfuseur-transfusé). L’analyse a été menée au moyen
were associated with the highest mean levels of hemoglobin in
des lignes directrices MOOSE. Les différences ont été considérées
anemic twins (P = 0.021), the lowest levels in polycythemic twins
significatives lorsque P < 0,05.
(P = 0.025), and the lowest frequency of postnatal procedures
(P < 0.001). Survival rate was independent of gestational age at Synthèse des données : Nous avons évalué des données portant sur
diagnosis and in utero therapy. In cases of TAPS following twin-to- 28 grossesses présentant une TAPS. Le diagnostic à 15-23 semaines
twin transfusion, the mean hemoglobin level was higher in donors de gestation et le traitement in utero ont été associés aux taux moyens
than in anemic twins with isolated TAPS (P = 0.029) and similar d’hémoglobine les plus élevés chez les jumeaux anémiques (P =
between recipients and polycythemic twins with isolated TAPS 0,021), aux taux moyens d’hémoglobine les plus bas chez les jumeaux
(P = 0.135). Twins with TAPS following twin-to-twin transfusion présentant une polyglobulie (P = 0,025) et à la fréquence d’interventions
received in utero therapy more frequently than isolated TAPS twins postnatales la plus basse (P < 0,001). Le taux de survie ne dépendait
(P = 0.030) and required a postnatal procedure less often ni de l’âge gestationnel au moment du diagnostic ni de la présence
(P < 0.001). Survival rates were similar in each group. d’un traitement in utero. Dans les cas de TAPS suivant le syndrome
transfuseur-transfusé, le taux moyen d’hémoglobine était plus élevé
Conclusion: Diagnosis of TAPS at an early gestational age is
chez les transfuseurs (par comparaison avec la situation constatée chez
associated with more favourable outcomes than later diagnosis. In
les jumeaux anémiques dans les cas de TAPS isolée [P = 0,029]) et il
utero therapy improves neonatal hemoglobin levels but does not
était semblable chez les transfusés (par comparaison avec la situation
change survival rates. Previous twin-to-twin transfusion syndrome
constatée chez les jumeaux présentant une polyglobulie dans les
does not worsen outcomes.
cas de TAPS isolée [P = 0,135]). Les jumeaux présentant une TAPS
constatée à la suite du syndrome transfuseur-transfusé ont reçu un
traitement in utero plus fréquemment (P = 0,030) et ont nécessité une
intervention postnatale moins souvent (P < 0,001) que les jumeaux
J Obstet Gynaecol Can 2014;36(8):701–707 présentant une TAPS isolée. Les taux de survie étaient semblables d’un
groupe à l’autre.
Key Words: Monochorionic pregnancy, twins, anemia Conclusion : L’établissement d’un diagnostic de TAPS à un âge
polycythemia sequence, twin transfusion syndromes gestationnel précoce est associé à des issues plus favorables que
l’établissement d’un diagnostic de TAPS à un âge gestationnel plus
Competing Interests: None declared.
tardif. L’administration d’un traitement in utero améliore les taux
Received on November 2, 2013 néonataux d’hémoglobine, mais ne modifie en rien les taux de survie.
Accepted on February 12, 2014 La présence d’un syndrome transfuseur-transfusé au préalable
n’aggrave en rien les issues.
AUGUST JOGC AOÛT 2014 l 701
Obstetrics
INTRODUCTION METHODS
T win anemia-polycythemia sequence is a specific
complication of monochorionic twin pregnancy. It
has been classified as isolated TAPS or TAPS associated
We searched PubMed, Embase, Medline, Clinicaltrials.org,
and reference lists to identify articles that described
perinatal outcomes of TAPS, from the inception of these
with twin-to-twin transfusion syndrome. Both TAPS and databases to November 2012. Key words used in the search
TTTS are typical features of monochorionic pregnancies. were twins, monochorionic pregnancies, twin anemia-
TTTS is characterized by polyhydramnios in the recipient polycythemia sequence, twin-to-twin transfusion syndrome,
sac and oligohydramnios in the donor sac, whereas TAPS placental anastomoses, recurrent TTTS, fetal anemia, and
is characterized by polycythemia in the recipient and fetal polycythemia. Each author independently selected
anemia in the donor twin, but amniotic fluid volume is articles, and discordance was resolved by consensus. The
normal in both sacs. These characteristics are used to MOOSE guidelines were followed. This meta-analysis was
distinguish between the two conditions. TAPS can occur based on case reports with raw data described for each case;
in isolation or may arise when laser therapy for TTTS the data were collected and pooled as a single large study.
is followed by the persistence of vascular anastomoses, Where data were missing, we attempted to contact the
leading again to anemia and polycythemia but with corresponding author to obtain unpublished data. When
normal amniotic fluid volumes.1 TAPS is diagnosed more than one article was published by the same authors,
prenatally by Doppler measurement of the peak systolic we selected the article with the largest sample size in order
velocity of the middle cerebral artery in each twin. PSV to avoid overlap of population. Overlap of population was
in the MCA > 1.5 MoM in one twin and < 0.8 MoM in assessed according to the authors and institution where the
the other are generally used to identify the anemic and study was performed and the year of publication.
polycythemic twin, respectively.2,3 Prenatal diagnosis is
confirmed at birth by measurement of each neonate’s Inclusion criteria for study selection were:
hemoglobin concentration, and thresholds of < 110 g/L 1. prenatal diagnosis of TAPS based on MCA-PSV
and > 200 g/L are applied for diagnosis of anemia
> 1.5 MoM in one twin and < 0.8 MoM in the second
and polycythemia, respectively.4 Postnatal TAPS can be
with normal amniotic fluid volumes, and
classified according to the criteria proposed by Lopriore,
which are based on differences in Hb levels between 2. confirmation of the diagnosis at birth with Hb levels
twins.5 The incidence of TAPS in monochorionic < 110 g/L for the anemic twin and > 200 g/L for the
pregnancies is estimated at 3% to 5% for the isolated polycythemic twin. Monoamniotic twin pregnancies
forms4 and at 2% to 13% after laser therapy for TTTS.3 were excluded.
Because of the relatively low incidence, the literature is
limited to the description of small series or case reports Outcomes of interest were Hb concentration and
of twins affected by TAPS. The aim of this review was reticulocyte count at birth, postnatal procedures, neonatal
to collect and pool published case reports of perinatal morbidity, and overall survival rates. Postnatal procedures
outcomes of TAPS identified prenatally, in order to comprised blood exchange in the polycythemic twin and
obtain a larger sample size. blood transfusion in the anemic twin. Overall survival rate
was defined as the number of survivors at least 28 days after
birth. Outcomes were stratified according to gestational
age at diagnosis of TAPS, performance of intrauterine
therapy, mode of onset, and presence of patent vascular
anastomoses on placental histological examination.
ABBREVIATIONS Gestational age at diagnosis was arbitrarily divided into
aTAPS TAPS following TTTS three intervals: 15 to 23 weeks, 24 to 29 weeks, and > 29
Hb hemoglobin weeks. Intrauterine therapy included laser therapy of
iTAPS isolated TAPS placental vascular anastomoses, blood transfusion by
MCA middle cerebral artery cordocentesis, and umbilical cord occlusion. The mode
MoM multiple of the median of onset consisted of isolated TAPS or TAPS associated
MVP maximum vertical pocket
with previous laser therapy for TTTS.
PSV peak systolic velocity We used the Mann-Whitney U, Kruskall-Wallis, and Fisher
TAPS twin anemia-polycythemia sequence exact test, as appropriate, in GraphPad Prism (GraphPad
TTTS twin-to-twin transfusion syndrome Software Inc., La Jolla CA) for statistical analysis. Statistical
702 l AUGUST JOGC AOÛT 2014
Perinatal Outcomes of Twin Anemia–Polycythemia Sequence: A Systematic Review
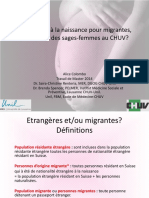
Flow chart for study selection
Potentially relevant observational Observatinal studies excluded
studies concerning perinatal because were not published during
outcomes of TAPS the study period
N = 1203 n = 407
Observational studies excluded based
Observational studies retrieved for on title or abstract (case reports,
more detailed evaluation reviews, personal communications)
n = 36 n = 14
Observational studies excluded
Potentially appropriate because did not meet the
observational studies to be inclusion criteria
included in the meta-analysis n = 12
n = 22
Observational studies with usable
information included in the
meta-analysis
n = 10
significance was reached with two-sided P values < 0.05. required in nine anemic twins (39%). The overall survival
We addressed quality issues in the description of studies rate was 82% (46/56); of these survivors, 50% (23/46) were
and in the discussion of findings. the anemic twin and 50% (23/46) were the polycythemic
twin. For each twin set, there were no survivors in 3%
RESULTS of pregnancies (1/28), one survivor in 28% (8/28),
and two survivors in 68% (19/28). Neonatal morbidity
The steps taken for study selection are shown in the Figure. affected five newborns (9%) and was represented by
Of 36 articles retrieved for detailed evaluation, 10 articles thrombocytopenia, neurologic disease, skin necrosis, mild
were selected for inclusion in the analysis; these described hypotonia, and respiratory distress. In two cases, neonatal
28 monochorionic twin pregnancies affected by TAPS (56 morbidity was fatal. Placental examination was performed
fetuses).1,3,6–13 The characteristics of each study are described in 11 of 28 pregnancies (39%) and revealed patent vascular
in Table 1. Median gestational age at diagnosis was 24 weeks anastomoses in seven (64%); two of these had previously
(range 15 to 33 weeks). In 17 pregnancies (61%), TAPS was undergone laser therapy for TTTS.
diagnosed after laser treatment of TTTS. Intrauterine therapy
was performed in 20 pregnancies (71%); this consisted of Diagnosis at 15 to 23 weeks’ gestation was associated with
laser treatment of placental vascular anastomoses (4 cases, more normal Hb levels. When TAPS was diagnosed at > 29
20%), blood transfusion in the anemic twin by cordocentesis weeks, conservative management was more likely than
(13 cases, 65%), and umbilical cord occlusion for impending with earlier diagnosis, but postnatal procedures were more
intrauterine death (3 cases, 15%). frequently performed. The overall survival rates did not
differ according to gestational age at diagnosis (Table 2).
At birth, the mean (± SD) Hb levels were 108.9 ± 54.4 g/L
and 203.7 ± 46.2 g/L in the anemic and polycythemic Comparison between TAPS treated in utero and
twins, respectively. Blood exchange was required in seven TAPS managed conservatively showed that the former
polycythemic twins (30%) and blood transfusion was significantly improved Hb levels at birth and reduced the
AUGUST JOGC AOÛT 2014 l 703
Obstetrics
Table 1. Characteristics of the studies
Type of GA at diagnosis In utero Residual Postnatal Survivors,
Author Cases TAPS of TAPS therapy anastomoses procedure n
Lopriore et al.12 Case 1 Isolated 15 No NA None 1
Groussolles et al. 8
Case 1 Associated 18 II Laser Absent None 2
Herway et al.10 Case 1 Associated 20 Transfusion Present E/T 2
Weingertner et al.13 Case 1 Isolated 32 No Present E/T 2
Case 2 Isolated 32 No Present E/T 2
Case 3 Isolated 32 No Present E/T 2
Case 4 Isolated 23 Laser Absent E/T 2
Gucciardo et al.9 Case 1 Isolated 26 Transfusion NA T 2
Case 2 Isolated 24 UCO NA T 1
Transfusion
Case 3 Isolated 29 Laser Absent None 2
Transfusion
Hemodilution
Fratelli et al. 7 Case 1 Associated 27 No Present E/T 2
Lopriore et al. 1
Case 1 Isolated 33 No Present T 2
Case 2 Isolated na No Present E/T 2
Robyr et al.3 Case 1 Associated 27 Transfusion NA None 2
Case 2 Associated 24 Transfusion NA None 2
Case 3 Associated 20 Transfusion NA None 1
Case 4 Associated 19 Transfusion NA None 1
Case 5 Associated 26 Transfusion NA None 2
Case 6 Associated 23 Transfusion NA None 1
Case 7 Associated 21 Transfusion NA NA 1
Case 8 Associated 25 UCO NA None 1
Case 9 Associated 23 Transfusion NA None 0
Case 10 Associated 22 Transfusion NA None 2
Case 11 Associated 24 Transfusion NA None 2
Case 12 Associated 18 Transfusion NA None 2
Case 13 Associated 28 Transfusion NA None 2
Lopriore et al. 11
Case 1 Associated 20 No Absent None 2
Assaf et al. 6 Case 1 Isolated 19 Laser NA None 1
UCO: umbilical cord occlusion; E: blood exchange in the polycythemic twin; T: blood transfusion in the anemic twin; NA: not available
Table 2. Outcomes according to gestational age at diagnosis of TAPS
Gestational age at diagnosis of TAPS
15 to 23 weeks 24 to 29 weeks 32 to 33 weeks
13 pregnancies 10 pregnancies 4 pregnancies
N (26 twins) (20 twins) (8 twins) P
Hb anemic twin, g/L, mean ± SD 146 ± 60.1 98.6 ± 35.1 60.7 ± 20.7 0.021
Hb polycythemic twin g/L, mean ± SD 171 ± 46.7 227 ± 34.1 216.8 ± 9.4 0.025
In utero therapy, n (%) 10/13 (77) 9/10 (90) 0/4 (0) 0.003
Overall survival, n (%) 18/26 (69) 18/20 (90) 8/8 (100) 0.068
Postnatal procedures, n (%) 4/26 (15) 4/20 (20) 7/8 (87) < 0.001
704 l AUGUST JOGC AOÛT 2014
Perinatal Outcomes of Twin Anemia–Polycythemia Sequence: A Systematic Review
risk of postnatal procedures. Survival rates did not differ secondary to polycythemia, closed small anastomoses.
significantly, either in overall survival or according to the Therefore, failure to demonstrate patent vessels on
number of surviving twins (Table 3). placental examination is not a requirement for excluding
the diagnosis of TAPS.
When compared with iTAPS, cases of aTAPS were treated
in utero more often and required postnatal procedures less We found that neonatal anemia and polycythemia do not
frequently. Gestational age at diagnosis of TAPS, Hb levels depend on the patency of vascular anastomoses. However,
at birth, and survival rates did not differ between the two in anemic neonates with patent placental anastomoses
groups. We observed more normal Hb levels in neonates detected by placental histological examination, the mean
after aTAPS than after iTAPS In Table 4, this comparison Hb was lower (85.1 g/L) than in anemic neonates without
is shown with twins classified as follows: patent anastomoses (167.5 g/L). This difference might
● Donor twin: donor twin with TAPS following TTTS be clinically relevant, although it did not reach statistical
treated with laser therapy significance (likely because of the small sample size).
● Anemic twin: donor twin with TAPS without previous The key limitation of our review was the paucity of
TTTS information available in the literature. Although we observed
● Recipient twin: recipient twin with TAPS following better outcomes for twins with TAPS treated in utero, there
TTTS treated with laser therapy are no standard criteria for selecting the initial treatment for
● Polycythemic twin: recipient twin with TAPS without TAPS. Doppler surveillance of the middle cerebral artery
previous TTTS every four weeks has been suggested,3 but the threshold
value for intervention has not been established. Intrauterine
Finally, the Hb levels were not influenced by the patency blood transfusion, laser ablation of placental anastomoses,
of vascular anastomoses (Table 5). umbilical cord occlusion, and expectant management have
been described,1,3,6–13 but the numbers in case series have
DISCUSSION been too small to compare the different methods. Moreover,
the limited number of cases in our dataset did not allow us
In this review we found that the overall survival rate in twins to perform multivariable analyses.
affected by TAPS was 82% and was similar for the anemic
and the polycythemic twin. Neonatal morbidity occurred Reticulocyte count is essential for the postnatal diagnosis
in 9% of cases, and in a very few it was severe enough to of TAPS,5 but in the articles we reviewed there was no
cause neonatal death. We also observed that more normal consensus about units or values. In fact, the reticulocyte
Hb levels at birth were related to early diagnosis (gestational count was reported as a percentage in some articles,10–12
age 15 to 23 weeks), probably because this allows specific as an absolute value in others,1,7–9,13 and was sometimes
management and intrauterine therapy. However, we noted unreported,3,6 making it impossible to pool data in a single
that survival rates increased from 69% to 100% in association meta-analysis.
with increasing gestational age at diagnosis.
TAPS associated with TTTS might have a different natural
In addition, previous TTTS did not worsen neonatal history from isolated TAPS, although the definition is
outcomes. Indeed, TAPS after laser therapy for TTTS was similar. Therefore, further studies are needed to clarify
associated with more normal Hb levels in both anemic what management and treatment should be performed for
and polycythemic twins than isolated TAPS. It may be these two entities.
speculated that laser therapy provides protection by
In our opinion, the main limitation of assessing conditions
reducing the severity of later TAPS.
associated with inter-twin transfusion is that it is still
It is generally believed that TAPS results from inter-twin difficult to determine when inter-twin blood exchange
blood transfusion through small vascular anastomoses.1 In becomes unequal. It is generally believed that blood
the cases in our review, placental histological assessment transfusion becomes pathological (and unequal) when a
(which should be mandatory in monochorionic twin twin oligo/polyhydramnios sequence develops. However,
pregnancies complicated by TAPS or TTTS) was performed the definition of oligo/polyhydramnios (MVP < 2 cm
in only 39%. Histological assessment did not reveal patent for oligohydramnios and > 8 cm for polyhydramnios) is
vascular anastomoses in 36% of the examined placentas. subjective,14 since to our knowledge there have been no
Because patent anastomoses are necessary for inter-twin studies comparing amniotic fluid volumes in normal and
transfusion, it is likely that thrombotic events, probably abnormal monochorionic twins. In addition, the definition
AUGUST JOGC AOÛT 2014 l 705
Obstetrics
Table 3. Outcomes according to prenatal management
Conservative
In utero therapy management
20 pregnancies 8 pregnancies
N (40 twins) (16 twins) P
Hb anemic twin, g/L, mean ± SD 129.1 ± 50.0 71.0 ± 43.5 0.011
Hb polycythemic twin, g/L, mean ± SD 190.3 ± 50.1 230.5 ± 20.1 0.018
Overall survival, n (%) 31/40 (77) 15/24 (62) 0.254
No survivors, n (%) 1/20 (20) 0/8 NS
1 survivor, n (%) 7/20 (35) 1/8 (12) 0.053
2 survivors, n (%) 12/20 (60) 7/8 (87) 0.502
Postnatal procedures, n (%) 6/40 (15) 12/24 (50) 0.004
NS: not significant
Table 4. Outcomes according to mode of onset
aTAPS iTAPS
17 pregnancies 11 pregnancies
N (34 twins) (22 twins) P
Hb donor vs. anemic twin, g/L, mean ± SD 130.5 ± 53.6 80.8 ± 42.9 0.029
Hb recipient vs polycythemic twin, g/L, mean ± SD 192.7 ± 53.5 221.9 ± 22.9 0.135
Hb donor vs polycythemic twin, g/L, mean ± SD 130.5 ± 53.6 221.9 ± 22.9 < 0.001
Hb recipient vs anemic twin, g/L, mean ± SD 192.7 ± 53.5 80.8 ± 42.9 < 0.001
GA at diagnosis of TAPS, weeks, mean ± SD 22.65 ± 3.23 26.50 ± 6.20 0.07
In utero therapy, n (%) 15/17 (88) 5/11 (50) 0.03
Overall survival, n (%) 27/34 (79) 19/22 (86) 0.723
No survivors, n (%) 1/17 (16) 0/11 NS
1 survivor, n (%) 5/17 (29) 3/11 (27) NS
2 survivors 11/17 (65) 8/11 (73) NS
Postnatal procedures 3/34 (9) 14/22 (64) < 0.001
Table 5. Hemoglobin levels according to patency of vascular anastomoses assessed by
placental examination
Patent No patent
anastomoses anastomoses
N 7 placentas 4 placentas P
Hb anemic twin, g/L, mean ± SD 85.1 ± 27.0 167.5 ± 26.1 0.072
Hb polycythemic twin, g/L, mean ± SD 209.4 ± 53.4 199.0 ± 55.1 0.412
706 l AUGUST JOGC AOÛT 2014
Perinatal Outcomes of Twin Anemia–Polycythemia Sequence: A Systematic Review
does not include gestational age. In a recent study REFERENCES
reporting percentiles of amniotic fluid volume in normal
monochorionic diamniotic twins, Dekoninck et al. found 1. Lopriore E, Middeldorp JM, Oepkes D, Kanhai HH, Walther FJ,
Vandenbussche FP. Twin anemia-polycythemia sequence in two
that from 15 to 37 gestational weeks, the MVP at the 2.5th monochorionic twin pairs without oligo-polyhydramnios sequence.
centile ranges from 2.01 to 2.83 cm.15 Therefore, using a Placenta 2007;28(1):47–51.
definition of oligohydramnios < 2 cm would miss cases 2. Klaritsch P, Deprest J, Van Mieghem T, Gucciardo L, Done E, Jani J, et al.
from 15 to 37 weeks. Similarly, polyhydramnios (MVP at Reference ranges for middle cerebral artery peak systolic velocity in
the 97.5th centile) was > 8 cm only from 23 to 31 weeks.15 monochorionic diamniotic twins: a longitudinal study. Ultrasound Obstet
Gynecol 2009;34(2):149–54.
Moreover, at any gestational age, out-of-range MVP was
never < 2 cm and > 8 cm at the same time, as required 3. Robyr R, Lewi L, Salomon LJ, Yamamoto M, Bernard JP, Deprest J, et al.
Prevalence and management of late fetal complications following
to define pathological inter-twin transfusion.14 We believe successful selective laser coagulation of chorionic plate anastomoses
that a better definition would be helpful to understand why in twin-to-twin transfusion syndrome. Am J Obstet Gynecol
some twins develop selective growth restriction, some the 2006;194(3):796–803.
twin oligo/polyhydramnios sequence, and some TAPS, 4. Lewi L, Jani J, Blickstein I, Huber A, Gucciardo L, Van Mieghem T, et al.
while most are normal. The outcome of monochorionic diamniotic twin gestations in the era of
invasive fetal therapy: a prospective cohort study. Am J Obstet Gynecol
2008;199(5):514. e1–8.
In addition, it has been suggested that the pathophysiology
of TAPS is the slow transfusion of blood through a few 5. Slaghekke F, Kist WJ, Oepkes D, Pasman SA, Middeldorp JM,
Klumper FJ, et al. Twin anemia-polycythemia sequence: diagnostic
small vascular anastomoses1. If inter-twin blood exchange criteria, classification, perinatal management and outcome. Fetal Diagn
becomes unequal, anemia and polycythemia develop, Ther 2010;27(4):181–90.
manifested by abnormal Doppler velocimetry of the 6. Assaf SA, Benirschke K, Chmait RH. Spontaneous twin anemia-
middle cerebral artery; however, amniotic fluid volume polycythemia sequence complicated by recipient placental vascular
remains normal in both sacs, indicating blood flow thrombosis and hydrops fetalis. J Matern Fetal Neonatal Med
2011;24(3):549–52.
depletion in the fetal brain but normal renal function.
Nevertheless, because cerebral impairment is the late stage 7. Fratelli N, Prefumo F, Zambolo C, Zanardini C, Fichera A, Frusca T.
Conservative management in a case of iatrogenic twin anemia-
of fetal distress, it is unlikely that cerebral impairment polycythemia sequence. Ultrasound Obstet Gynecol 2012;39(5):597–8.
would occur before impairment of renal function. 8. Groussolles M, Sartor A, Connan L, Vayssiere C. Evolution of middle
cerebral artery peak systolic velocity after a successful laser procedure
We suggest that these conditions may be considered as a for iatrogenic twin anemia-polycythemia sequence. Ultrasound Obstet
single entity and probably occur in sequence: Gynecol 2012;39(3):354–6.
● No inter-twin transfusion of blood: normal twins 9. Gucciardo L, Lewi L, Vaast P, Debska M, De Catte L, Van Mieghem T,
et al. Twin anemia polycythemia sequence from a prenatal perspective.
● Mild inter-twin transfusion: selective intrauterine Prenat Diagn 2010;30(5):438–42.
growth restriction 10. Herway C, Johnson A, Moise K, Moise KJ Jr. Fetal intraperitoneal
transfusion for iatrogenic twin anemia-polycythemia sequence after laser
● Moderate inter-twin transfusion: abnormal renal therapy. Ultrasound Obstet Gynecol 2009;33(5):592–4.
function leading to amniotic fluid discordance (TTTS)
11. Lopriore E, Hecher K, Vandenbussche FP, van den Wijngaard JP,
● Severe inter-twin transfusion: abnormal cerebral Klumper FJ, Oepkes D. Fetoscopic laser treatment of twin-to-twin
perfusion (TAPS). transfusion syndrome followed by severe twin anemia-polycythemia
sequence with spontaneous resolution. Am J Obstet Gynecol
2008;198(2):e4–7.
Because of the relatively low incidence of monochorionic
twin pregnancies and related complications, large 12. Lopriore E, Slaghekke F, Kersbergen KJ, de Vries LS, Drogtrop AP,
Middeldorp JM, et al. Severe cerebral injury in a recipient with
multicentre studies are needed in order to investigate the twin anemia-polycythemia sequence. Ultrasound Obstet Gynecol
natural history of monochorionic twins. 2013;41(6):702–6.
13. Weingertner AS, Kohler A, Kohler M, Bouffet N, Hunsinger MC,
CONCLUSION Mager C, et al. Clinical and placental characteristics in four new cases
of twin anemia-polycythemia sequence. Ultrasound Obstet Gynecol
Improved hematological outcomes in both the anemic and 2010;35(4):490–4.
polycythemic twins affected by TAPS are associated with 14. Quintero RA, Morales WJ, Allen MH, Bornick PW, Johnson PK,
Kruger M. Staging of twin-twin transfusion syndrome. J Perinatol
early gestational age at diagnosis, intrauterine therapy, and 1999;19(8 Pt 1):550–5.
previous laser therapy for TTTS. Due to the low incidence
15. Dekoninck P, Deprest J, Lewi P, Richter J, Galjaard S, Van Keirsbilck J,
of TAPS, large multicentre studies would be useful to et al. Gestational age-specific reference ranges for amniotic fluid
develop standards for the management of twins affected assessment in monochorionic diamniotic twin pregnancies. Ultrasound
by TAPS. Obstet Gynecol 2013;41(6):649–52.
AUGUST JOGC AOÛT 2014 l 707
Vous aimerez peut-être aussi
- Le Dépassement de TermeDocument4 pagesLe Dépassement de TermeBouloulou DocPas encore d'évaluation
- Cat Devant Une RamDocument3 pagesCat Devant Une RamKILAS GERARDPas encore d'évaluation
- Grossesse FCS T1Document6 pagesGrossesse FCS T1Kpossou ibourahimPas encore d'évaluation
- Cours PSGADocument10 pagesCours PSGAsaid madaniPas encore d'évaluation
- Risk of UterineDocument5 pagesRisk of UterinerosmiaPas encore d'évaluation
- Dgo Prepa NaissanceDocument26 pagesDgo Prepa Naissancemonica y AlainPas encore d'évaluation
- Accouchemnt GemellaireDocument6 pagesAccouchemnt GemellaireKILAS GERARDPas encore d'évaluation
- Fiches - Pédagogiques - 2ème Année - Français - Ab - Final-1Document109 pagesFiches - Pédagogiques - 2ème Année - Français - Ab - Final-1tchiegang cynthiaPas encore d'évaluation
- Rapport OFSP Annexe-1 WebDocument86 pagesRapport OFSP Annexe-1 Webmonica y AlainPas encore d'évaluation
- MemoireDocument30 pagesMemoirebazelais kerving kPas encore d'évaluation
- ANCPNC Manuel Du FaciliteurDocument204 pagesANCPNC Manuel Du FaciliteurGasnicka BeltinordPas encore d'évaluation
- Retard de Croissance Intra Uterin M1 2014Document20 pagesRetard de Croissance Intra Uterin M1 2014Serge TresorPas encore d'évaluation
- Ornella L2GIS Corrigé BonDocument91 pagesOrnella L2GIS Corrigé Bonornellabimuloko53Pas encore d'évaluation
- Eclampsie en ReanimationDocument29 pagesEclampsie en ReanimationEbePas encore d'évaluation