Vous aimerez peut-être aussi
- Le Langage HTMLDocument11 pagesLe Langage HTMLAsmaPas encore d'évaluation
- Canon Rreurs Pixma G 2411Document5 pagesCanon Rreurs Pixma G 2411Saad HaderbachePas encore d'évaluation
- Delivrance: Renouvellement: Prorogation: Validation: Qualification: ConversionDocument5 pagesDelivrance: Renouvellement: Prorogation: Validation: Qualification: Conversionondajacques ondajacquesPas encore d'évaluation
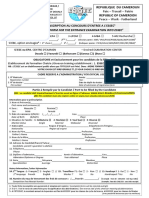
- p07 - Ce - Ngouagnia Kaffo Idriss NikerDocument1 pagep07 - Ce - Ngouagnia Kaffo Idriss NikerSang Amère IIPas encore d'évaluation
- TADH Job Application FormDocument5 pagesTADH Job Application FormClaire DelimaPas encore d'évaluation
- CV Format OBR Verificateurs Impots Et DouanesDocument5 pagesCV Format OBR Verificateurs Impots Et DouanesSavin ConayisavyePas encore d'évaluation
- Captura de Tela 2023-06-02 À(s) 14.26.20Document1 pageCaptura de Tela 2023-06-02 À(s) 14.26.20Sara GomesPas encore d'évaluation
- CV Format OBR-2022Document5 pagesCV Format OBR-2022Karikumutima TheobardPas encore d'évaluation
- F Renseignements Rentree2023-2024 ViergeDocument4 pagesF Renseignements Rentree2023-2024 ViergeelyoussoufiselmaPas encore d'évaluation
- Bourses Enseignement Gouv ci/img/dossiers/ATTFORMULAIRE20202021 PDFDocument2 pagesBourses Enseignement Gouv ci/img/dossiers/ATTFORMULAIRE20202021 PDFbenarjun100% (1)
- Fiche Inscription 2020-2021Document2 pagesFiche Inscription 2020-2021Bertrand Soppo YokiPas encore d'évaluation
- Nada EsgciDocument6 pagesNada Esgcinpc3405Pas encore d'évaluation
- ATTFORMULAIRE2223Document2 pagesATTFORMULAIRE2223Losseni KabaPas encore d'évaluation
- PSB - Free Mover - Study Abroad - Application FormDocument5 pagesPSB - Free Mover - Study Abroad - Application FormOcean CretPas encore d'évaluation
- Modele Grille Entretien Professionnel MOBEDocument4 pagesModele Grille Entretien Professionnel MOBEVeronique MobePas encore d'évaluation
- LE PRIX DE L'ETUDIANT ENTREPRENEUR 2024 SaNOSPRO 1Document1 pageLE PRIX DE L'ETUDIANT ENTREPRENEUR 2024 SaNOSPRO 1arsenewebsolutePas encore d'évaluation
- Formation Continue: Bulletin D'InscriptionDocument1 pageFormation Continue: Bulletin D'InscriptionMbatchi mavoungou RodriguePas encore d'évaluation
- Template CV CompletDocument11 pagesTemplate CV CompletMohamed AchrafPas encore d'évaluation
- Attformulaire2122 PDFDocument2 pagesAttformulaire2122 PDFFranck Bi baleyPas encore d'évaluation
- Demande Permis-FranceDocument2 pagesDemande Permis-Franceolivier BILLAUDETPas encore d'évaluation
- Bulletin D'Inscription: Offre de Stage PED #00 2/FONEA/2023Document1 pageBulletin D'Inscription: Offre de Stage PED #00 2/FONEA/2023Nik LavhiePas encore d'évaluation
- Mba Esg Dossier Candidature Mba 2ansDocument6 pagesMba Esg Dossier Candidature Mba 2ansaichatakan53Pas encore d'évaluation
- Questionnaire Demande de Qualification Toutes SpecialitesDocument8 pagesQuestionnaire Demande de Qualification Toutes Specialitesaurelie bringerPas encore d'évaluation
- PI Fiche Dinscription Reinscriptio N Système National 2022 2023Document1 pagePI Fiche Dinscription Reinscriptio N Système National 2022 2023emmanuel olaboPas encore d'évaluation
- Enabel Formulaire de Candidatures de Bourse de Master 2 202308Document10 pagesEnabel Formulaire de Candidatures de Bourse de Master 2 202308abdoulkarimrabiou10Pas encore d'évaluation
- Admission Eni AbtDocument4 pagesAdmission Eni AbtSouleymane Coulibaly100% (2)
- Fiche D'inscription Ifppdl 2Document1 pageFiche D'inscription Ifppdl 2Stéphane OhambaPas encore d'évaluation
- Demande Recevabilite VAEDocument4 pagesDemande Recevabilite VAEJM KoffiPas encore d'évaluation
- Formulaire Attribution de Bourse 2022Document2 pagesFormulaire Attribution de Bourse 2022amara joe syllaPas encore d'évaluation
- Fiche Dinscription Au Concours 1 2 2020 FRDocument2 pagesFiche Dinscription Au Concours 1 2 2020 FRPatrice Ngazanga AyissiPas encore d'évaluation
- Annex 1 GPP Personal History Profile Form (FR)Document5 pagesAnnex 1 GPP Personal History Profile Form (FR)snhcdtanaPas encore d'évaluation
- Fiche-Accueil-Clients-2023-À-Complétée Directement.Document2 pagesFiche-Accueil-Clients-2023-À-Complétée Directement.Marckdany NPas encore d'évaluation
- Demande de Vérification Des Dossiers de Police - UnitÉ RégionaleDocument2 pagesDemande de Vérification Des Dossiers de Police - UnitÉ RégionalepassioncadetPas encore d'évaluation
- Application FormDocument3 pagesApplication FormHalil JawPas encore d'évaluation
- Tarun Das CV For Gambia in AFDB FormatDocument15 pagesTarun Das CV For Gambia in AFDB FormatProfessor Tarun Das100% (1)
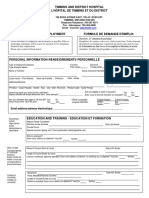
- PPD DemandeEmploi PDFDocument4 pagesPPD DemandeEmploi PDFIlyassBahaaPas encore d'évaluation
- Capture D'écran . 2022-11-24 À 6.58.06 PMDocument2 pagesCapture D'écran . 2022-11-24 À 6.58.06 PMPrisca DemosthenePas encore d'évaluation
- CSM Admi Form 2019V1Document2 pagesCSM Admi Form 2019V1abass diopPas encore d'évaluation
- Mba Esg Dossier Candidature Mba 2ansDocument6 pagesMba Esg Dossier Candidature Mba 2ansDylan FroissartPas encore d'évaluation
- 2020 DDR Vae 1Document14 pages2020 DDR Vae 1Sara ArezkiPas encore d'évaluation
- Dossier de CandidatureDocument3 pagesDossier de CandidatureIan NgounePas encore d'évaluation
- Fiche Dinscription Au Concours ESSEC 2022 Registration Form CEE ESSEC 2022Document2 pagesFiche Dinscription Au Concours ESSEC 2022 Registration Form CEE ESSEC 2022Boris ThierryPas encore d'évaluation
- Demande Pole EmploiDocument5 pagesDemande Pole EmploiVickyPas encore d'évaluation
- 51 Sous Dossier D Inscription ITICDocument4 pages51 Sous Dossier D Inscription ITICbondass23Pas encore d'évaluation
- 91 PDFDocument4 pages91 PDFKhaled BriberPas encore d'évaluation
- 08 2022 Dossier de CandidatureDocument4 pages08 2022 Dossier de Candidatureamougouzacharie84Pas encore d'évaluation
- IMM5658FDocument1 pageIMM5658FAhmed MIMOUNIPas encore d'évaluation
- Demande Admission Eleves Internationaux 02 22Document1 pageDemande Admission Eleves Internationaux 02 22nenkalangaPas encore d'évaluation
- Demande Admission Eleves Internationaux 02 22Document1 pageDemande Admission Eleves Internationaux 02 22Farid BelloPas encore d'évaluation
- Promesse D'embauche 2023 v2Document1 pagePromesse D'embauche 2023 v2mehdiismaili57Pas encore d'évaluation
- Imprimer FicheDocument1 pageImprimer FicheangelioneldigbeuPas encore d'évaluation
- Formulaire D'admission ESSIREMDocument5 pagesFormulaire D'admission ESSIREMsmartengineering457Pas encore d'évaluation
- Form - Adm - Eleves Etrangers 22 Remplissablel 2Document1 pageForm - Adm - Eleves Etrangers 22 Remplissablel 2Kęvīn TåmbôūPas encore d'évaluation
- Formulaire Demande de Préadmission Élève ÉtrangerDocument1 pageFormulaire Demande de Préadmission Élève ÉtrangerPa Xalilu JohnPas encore d'évaluation
- Demande de Pré-Enrôlement / Pre-Enrolment Application Passeport Ordinaire / Ordinary PassportDocument1 pageDemande de Pré-Enrôlement / Pre-Enrolment Application Passeport Ordinaire / Ordinary PassportBrice TchokotcheuPas encore d'évaluation
- E Rec Dossier Candidature (1) 2Document2 pagesE Rec Dossier Candidature (1) 2Soliman BrahimiPas encore d'évaluation
- HR Fo 006 v07 Demande D'emploiDocument2 pagesHR Fo 006 v07 Demande D'emploimariaPas encore d'évaluation
- Fiche de CandidatureDocument1 pageFiche de Candidatureservice solutionPas encore d'évaluation
- Dossier de Candidature EssemDocument4 pagesDossier de Candidature EssemAlseny CissePas encore d'évaluation
- Fo-daf-623-Demande de Creation de Matricule Sifac 1Document1 pageFo-daf-623-Demande de Creation de Matricule Sifac 1Ananya PulgamPas encore d'évaluation
- Dossier Candidature LyonDocument6 pagesDossier Candidature Lyonsandrinechaab74Pas encore d'évaluation
- Prog S2 HTML - CSS - BootstrapDocument102 pagesProg S2 HTML - CSS - BootstrapMalik SokorePas encore d'évaluation
- Recherche ScientifiqueDocument16 pagesRecherche Scientifiquecharte nyemba100% (1)
- Présentation Plateforme SéminairesDocument69 pagesPrésentation Plateforme SéminairesYolam VavaPas encore d'évaluation
- Exemplaire de CV en Arabe PDFDocument2 pagesExemplaire de CV en Arabe PDFMichaelPas encore d'évaluation
- Redigez Des Documents de Qualite Avec Latex PDFDocument220 pagesRedigez Des Documents de Qualite Avec Latex PDFkago1Pas encore d'évaluation
- Rib LexoiDocument1 pageRib Lexoikarim.nefra1Pas encore d'évaluation
- Théorie TDI FF CorrectionDocument7 pagesThéorie TDI FF CorrectionrzegergPas encore d'évaluation
- Rapport Bibliographique-Pages-SuppriméesDocument13 pagesRapport Bibliographique-Pages-SuppriméesChaoukiMatimaticPas encore d'évaluation
- Lettre Motivation Agent Postal CommunalDocument2 pagesLettre Motivation Agent Postal CommunalkengnePas encore d'évaluation
- DTL Chiffres RomainsDocument2 pagesDTL Chiffres Romainsboubacarmballo205Pas encore d'évaluation
- Guide PFEDocument22 pagesGuide PFEBouraoui Ben AyedPas encore d'évaluation
- SERIES TD 1 Et 2 LCSDocument2 pagesSERIES TD 1 Et 2 LCSnait amara zaidPas encore d'évaluation
- Enseigner: Avec Les Voisins Du 12 BisDocument117 pagesEnseigner: Avec Les Voisins Du 12 Bisbelen ortega ortuñoPas encore d'évaluation
- Réal de Montréal Cahier 1Document119 pagesRéal de Montréal Cahier 1Naïsène OuiouiPas encore d'évaluation
- Lipro - TD Web DesignDocument25 pagesLipro - TD Web DesignFFFFPas encore d'évaluation
- TP PythonDocument14 pagesTP PythonYouness ChadilyPas encore d'évaluation
- DAVO FR 2022 2023Document32 pagesDAVO FR 2022 2023Christian VPas encore d'évaluation
- Evaluation Math 3e Me Pe RiodeDocument6 pagesEvaluation Math 3e Me Pe RiodealainestorPas encore d'évaluation
- Cours 1Document9 pagesCours 1moustansir484Pas encore d'évaluation
- Titi Fricoteur Le Coq Du Village 2907682199Document1 pageTiti Fricoteur Le Coq Du Village 2907682199ehouarnPas encore d'évaluation
- Correction VSLAM AsymetriqueDocument4 pagesCorrection VSLAM Asymetriquesellami100% (1)
- Revision DS - SOA (XML)Document14 pagesRevision DS - SOA (XML)chadha hidriPas encore d'évaluation
- Livre ÉpuiséDocument6 pagesLivre ÉpuiséArthur LecoqPas encore d'évaluation
- Guides de La Documentation Ecrite 2022-2023Document163 pagesGuides de La Documentation Ecrite 2022-2023Simon DelanayePas encore d'évaluation
- Résumé Mobile Codename OneDocument8 pagesRésumé Mobile Codename OneNihed AttiaPas encore d'évaluation
- Chapitre 4 - Les Chaines de CaractèresDocument7 pagesChapitre 4 - Les Chaines de CaractèresTarhôùni HosnïPas encore d'évaluation
- Web Sémantique Et Ontologie (WSO) : Rapport de TP N°1Document9 pagesWeb Sémantique Et Ontologie (WSO) : Rapport de TP N°1فركوس محمد العيدPas encore d'évaluation
- 2 Codage & NumérationDocument54 pages2 Codage & NumérationFatima Ezzahra MarzaouiPas encore d'évaluation