Académique Documents
Professionnel Documents
Culture Documents
SINTROM
Transféré par
Iin NurCopyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
SINTROM
Transféré par
Iin NurDroits d'auteur :
Formats disponibles
.,.
2d72
MAYER AND CONNELL: SINTROM
Canad. M. A. J. Feb. 15, 1957, vol. 76
8. KANOF, A., KRAMER, B. AND CARNES, M.: J. Pediat., 14: 712, 1939. 9. BOWMAN, W. D.: Personal communication, 1953. 10. MARTIN, W. J. et al.: Proc. Staff Meet. Mayo CliGu.. 29: 379, 1954. 11. TAYLOR, W. J.: Personal communication, 1954. 12. GARROD, L. P. AND WATERWORTH, P. M.: Brit. M. J., 2: 61, 1956.
1. It is emphasized that this disease occurs in infants and young children. 2. The danger of hospital infection is noted. 3. The mortality rate was high (44%). 4. The frequency of complications has been shown. 5. The ineffectiveness of most antibiotics has been noted. 6. The value of nasal swabs is noted.
My thanks are due to Professor Harry Dr. I. Graham.
REFERENCES
RESUME
L'auteur rapporte ici les observations qu'il a ete 'a menme de faire en traitant 27 cas de pneumonie ai staphylocoques chez des enfants dont la majorit, etait agee de 3 mois ou moins. Plusieurs d'entre eux avaient souffert d'infections 'i staphylocoques anterieurement, soit au niveau de la peau ou au niveau du tube digestif. Neuf de ces petits malades montrerent tres peu de signes cliniques 'a l'admission. Des complications surgirent dans 22 cas, et le taux de mortalite s'eleva La 44.4%. La grande majorite des souches de staphylocoques dores obtenues dans ces cas etait resistante 'a la plupart des antibiotes sauf le chloramphenicol et l'erythromycine. Comme dans plusieurs autres hopitaux, on isola des staphylocoques resistants des voies nasales de 84% dui personnel employe au departement de maternite. Ces observations confirment celles contenues dans d'autres articles sur le meme sujet dejLa parLs dans cette revue. M.R.D.
Mledovy
and
65: 439, 1951. 2. KANOF, A. et al.: Pediatrics, 11: 385, 1953. 3. BLOOMER, W. E. et al.: J. Thoracic Sury., 30: 265, 1955. 4. BEAVEN, D. W. AND BURRY, A. F.: Lancet, 2: 211, 1956. 5. RODGERS, D. E. et al.: Ann. New York Acad. Sc., 65: 57, 1956. 6. GUTHRIE, K. J. AND MONTGOMERY, G. L.: Lancet, 2: 752, 1947. 7. MACAULAY, D.: Ai-ch. Dis. Child., 27: 107, 1952.
1. DE PAPE, A. J. AND MCEWEN, D. S.: Catnad. M. A. J.,
THE ANTICOAGULANT EFFECT OF A NEW COUMARIN DERIVATIVE - SINTROM (GEIGY)AND ITS CONTROL BY STANDARDIZED CLOTTING TIME*
GEORGE A. MAYER, M.D. and W. FORD CONNELL, M.D., Kingston, Ont.
IN A PREVIOUS PAPER, we demonstrated a consistent relationship between dicoumarol therapy and the clotting time of unmodified whole blood measured by a standardized procedure.1 Clinical observation and statistical analysis of our data showed that this might be a more reliable method of controlling dicoumarol therapy than the Quick one-stage prothrombin test. In this study the daily prescription of dicoumarol was governed largely by prothrombin values - the standardized clotting time being registered only for purposes of our research. We now report the result of anticoagulant therapy in 42 patients, controlled solely by the standardized clotting time. The anticoagulant used in this study was 3 - [a(44 nitrophenyl) -,facetylethyl] - 4 oxycou*From the Departmenit of NIedicine, Queen's University and the Kingston General Hospital. This study was supported by the J. P. Bickell Foundation, Toronto. The heparin was supplied by the Coninaught Medical Research Laboratories, Toronto.
marin (Sintrom) t, a new coumarin derivative synthesized by Stoll and Litvan.2 Considerable information is already available on this drug. Milligram for milligram, it is 25 times as potent as is phenylindandione3 and 40 times as potent as Tromexan.4 After its administration, factor VII and prothrombin are decreased in amount; factor V is unaffected.4 A prothrombin level of 30%o could be attained in from 24 to 72 hours after the first dose.5 Weiner; and his colleagues have recently reported this drug to act somewhat more rapidly than dicoumarol but more slowly than Tromexan. Prothrombin time was shown to return to normal in from 24 to 48 hours after the drug was discontinued. No toxic effects or gastro-intestinal disturbances were reported in either animals or humans when doses were kept in the usual therapeutic range. Early workers'5 recommended a starting dose of 28 mg., 20 to 24 mg. on the second day, and 12 to 20 mg. on the third. Thereafter, prothrombin time was used to regulate dosage. Of the 42 patients we treated, 22 had acute myocardial infarction (15 "poor risk" cases), 12 had acute coronary insufficiency, three pulmonary embolism, four peripheral thrombophlebitis and one cerebral embolism.
tSintromn was stupplied by Geigy Pharimiacetiticals l,td., Monit real.
Canad. M. A. J. Feb. 15, 1957, vol. 76
MAYER
AND
CONNELL: SINTRoM 273
METHODS
1. Standardized clotting time (SCT) was measured on unmodified venous blood immediately after withdrawal, following the method of Mayer.7 Readings were expressed in minutes. Normal values were 9.69 + 0.55 minutes. 2. The Quick one-stage prothrombin test8 was performed in the laboratories of the Kingston General Hospital within two hours of blood withdrawal. Each day fresh Difco BactoThromboplastin (dried rabbit brain) was used. The daily normal prothrombin time varied between 13 and 16 seconds. Prothrombin activity in per cent (PTR) was calculated from the dilution curve of pooled normal human plasma. Blood for both tests was taken in the morning. Patients were not always in the fasting state.
Sintrom was started on the first day, with a dose of 20 to 24 mg. On each of the following three days we reduced the dose by 4 mg.-the total dose for the day being given at noon, after food. Thereafter, the dosage of Sintrom was adjusted to maintain SCT readings in our therapeutic range of between 15 and 20 minutes. PTR was registered for purposes of comparison only. All patients received 500 mg. of ascorbic acid daily throughout anticoagulant therapy. Other drugs were administered as was dictated by the clinical course.
RESULTS The anticoagulant treatment of these 42 patients was studied for a total of 866 treatment
TABLE I.-STANDARDIZED CLOTTING TIME (SCT) DURING SINTROM THERAPY
Days
n
Mean
1
10
11
12
1s
14
15
16
17
18
19
20
40
10.70
39
12.41
*0.41
41
14. 27 *0. 43
40
42
41
17.83
*0. 64
38
17.97 3 .90
*0. 63
36
18. 69
56
18.1
33
17.87 *0.63
28
17.03 68
27
16.25
26
18.07
22
17.27 *0.85 23.3
24
16.7 *0. 79
23.4
19
17.52
18
17.11 *0. 77 19.2
19
16.94 *0.64
16.5
15
18.00 0. 97 20.7
12
18.41 22 23.0
14
17.21
1 14
SD
*1.
1. 55 *2.57 *2.80
20.7
19.7
SE .0. 24
C*
.14 5
15.92 16.85 3 3 *0. 58 *0. 58 22.6 23.3
.71
.81 *4.15
23.3
*1=3.38*3.60 3.61
20.1
21.2
3.801
*4.60
*0.90
25.5
4.031
*3.90 *2.06 3.29 2.80*3.72 4.25 4 25
*0. 47 11.8
*0. 73
23.4
21.7
24.7
*Coefficient of variation in per cent.
TABLE II.-PRoTHROMBIN (PTR) ACrivITY (QUICK ONE-STAGE METHOD) DURING SINTROM THERAPY
Days
n
1
10
11
12
13
14
15
16
17
18
19
20
42 42 41 42 41 31 26 28 26 20 22 39 35 18 18 19 16 Mean 58.00 26.57 18.3 20.43 21.14 21.73 22.76 25.97 31.61 30.73 33.00 30.92 37.1 41.54 35.72 34.55 36.26 32.06 SD *16.7 *13.09 *14.03 *16.1 *16.6 *12.7 *14.0 *15.5 *19.4 *20.3 *17.7 *20.66 *18.8 *16.7 *11.5 *16.2 *16.6 *13.2 SE *2.6 *2.02 *2.16 *2.51 *2.56 *1.98 *2.24 *02.62 *3.48 *3.98 *3.34 *9.05 *1.22 *3.56 *2.71 *3.82 *3.81 *3.3 C* 76.7 78.8 78.5 58.4 61.5 59.7 61.4 66.1 53.6 28.8 49.3 66.8 50.7 40.2 32.2 46.9 45.8 41.2 *Coefficient of variation in per cent.
41
*10.891=17.6 *3.336.1
11 30.18
13 39.30
*4.88
41.8
TREATMENT
Anticoagulant therapy was initiated in all cases by the intravenous administration of 100 mg. heparin; this dose was repeated approximately seven-hourly during the daytime thereafter. The usual times of injection were 9 a.m., 4 p.m. and 11 p.m. Blood tests were taken each morning 9 to 10 hours after the bedtime dose and always before the morning dose of heparin. This schedule was maintained until the SCT attained approximately 14 minutes, when the daily heparin dosage was reduced to 100 mg. b.i.d. (injections at 10 a.m. and 10 p.m.). When the SCT reached the 15-16 minute level, heparin was discontinued. In rare instances the effect of heparin was unduly prolonged; this was detected easily by maintained rise of SCT (Fig. 3) and the subsequent doses of heparin' were adjusted or entirely omitted.
days. On 18 of these days heparin only was administered, and for 128 days heparin and Sintrom were given concurrently. For 720 treatment days Sintrom was the only anticoagulant given. Statistical analysis of the SCT readings showed a slow, steady rise of the arithmetic mean (Table I) until the eighth day, when the 18-minute level was attained. The mean remained approximately at this level during the subsequent days. The coefficient of variation was approximately 20% throughout the study. The corresponding mean of the PTh (Table II) showed a very rapid decrease. In from 36 to 48 hours after the first Sintrom dose it was 26%, and on the third day 18%. It remained around this level until the ninth day, when it rose to 30%, and on the 13th day to 37%, varying thereafter from 30 to 40%. The wide variation in individual IPTR readings is shown by the high coefficients of variation.
274 MAYER AND CONNELL: SINTROM
Canad. M. A. J. Feb. 15, 1957, vol. 76
PTR
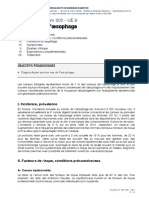
with adequate SCT prolongations. Later, on the 21st day, 60%--20, _ _ a similar PTR value was asso70 Y0* -ciated with an excessively high 80% -10 SCT value (33 minutes). On the average, 4.3 days 6 4 10 12 14 16 0 2 8 were required to attain an 18 20 DAYS Fig. 1.-Curves of means of SCT and PTR (Quick one-stage method) in SCT of 15 minutes. Individual 42 patients under Sintrom therapy. Note the rapid decrease of PTR and slow cases exhibited marked variacssehbtd'akdvra rise of SCT. tions in the rapidity of- the Correlation coefficients between SCT and PTR onset of adequate SCT levels (Table III). A varied from -0.1 to -0.47. PTR level of 30% was reached on the average The curves of the means J. E. d' 37 Y CORONARY INSUFFICIENCY (Fig. 1) show a lag of SCT as compared with PTR during p;R the first nine days of therapy. 0 Thereafter, they run more or CT mi. 10 % less parallel. We found several cases exhibiting marked PTR 20 % 40 , depression with therapeutic . %. SCT levels (Fig. 2).' In other 40% 30 cases similar SCT readings 50 % were maintained with very 70 % 20 moderate depression of PTR
40 %- -30
20 % 40 30% t r
10% SCT min.
PTR
mean
_ -
'~'
same patients. A case is illus<10% |trated (Fig. 2) in which PTR values of less than 109% were noted for six days at the be-
ginning of Sintrom therapy
S5T
SYMBOLS {| 100mg HEPARIN I.V. 90 % In 21 cases PTR readings of IEII.EI ,. . .' . 6 j6 6 ,616 100 % 0 2 4 6 8 10 12 14 16 18 20 DAYS under 10% were recorded on Fig. 3.-Therapeutic SCT prolongation with moderate PTR depression in two or more days in the first a 37-year-old male patient with coronary insufficiency. Note the high SCT reading 10 days of therapy. Such the SCT on the third day. Omission of heparin resulted in a rapid decrease of the following day. marked PTR depression with therapeutic values of SCT was not a common in 2.2 days. Thirty patients attained this level feature after the second week of therapy in the within two days, 10 in three days (Table IV). The speed of attainment of J. S.9 74Y. CORONARY INSUFFICIENCY adequate SCT levels was not DIABETES MELLITUS found to be accelerated by PTR 110' 131? 72' 64! 92further increases of the initial O0% doses within reasonable limits. 10 % SCPTRi e 20 % - 4 ' The analysis of the period 30 when Sintrom was the sole 40 % - 30 anticoagulant shows that our therapeutic aim to keep SCT % between 15 and 20 minutes 0 4mg SINTROM so % * was achieved in 71% of treatTHERAPY 90 % . ,o ,oSYMBOLS IOOmg HEPARIN LV. ment days (Table V). On 15% to 10 16 16 to 11 18 1007.0 4 6 8 10 12 14 16 20 24 DAYS of treatment days SCT was less Fig. 2.-Sintroma therapy of a 74-year-old female patient with acute corothan 15 minutes, on 12%G it nary insufficiency. Marked PTR depression with moderate prolongation of SCT at the beginning of treatment. On the 21st day a similar PTR reading was was between 21 and 25 minassociated with a very high SCT.
0
(Fig. 3.)THRP
74
93
<I
," _ . _ * _ ^._ __
WA
I
.
I
50%
,8
.0
iw
.0
.0
.10
.0
Is
22
Canad. M. A. J. Feb. 15, 1957, vol. 76
MAYER AND CONNELL: SINTROM 275
DURATION OF EFFECT OF DRUG
-
TABLE III.-NUMBER OF DAYS REQUIRED TO ATTAIN SCT OF 15 MINUTES AFTER THE FIRST DOSE OF SINTROM No. of No. of cases days %
1
2 3 4 5 6 7 8 9 never Average
7 8 6 8 4 4 1 1 2
16.7 19.0 14.4 19.0 9.5 9.5 2.4 2.4 4.8 4.3 days.
2.3
In 26 cases we followed the changes of SCT and PTR after cessation of Sintrom therapy. Both tests returned to pre-treatment levels within two days in 12 cases, within three days in 11, and in four days in three cases.
COMPLICATIONS The drug was well tolerated by all the
utes, and on 2%, between 26 and 30 minutes. The parallel PTR readings (Table V) varied widely. We have recorded 15 days when the SCT was markedly above our safety limit-i.e., between 26 and 30 minutes. PTR values for these 15 days were as follows: one less than 10%; four between 10 and 20%; eight between 21 and 30%o; two between 31 and 40%. On one occasion we noted SCT above 31 minutes with a corresponding PTR of less than 10%.
TABLE IV.-NUMBER OF DAYS REQUIRED TO ATTAIN A PTR ACTIVITY OF 30% AFTER THE FIRST DOSE OF
SINTROM No. of No. of cases days TO 7.1 1 3 64.3 2 27 24.0 10 3 1 4 2.3 1 2.3 never Average 2.2 days.
patients. No gastro-intestinal or other disturbances ascribable to Sintrom administration were observed. We encountered one minor bleeding-epistaxis, requiring a gauze pack. This occurred when the SCT was 25 minutes and the PTR 24%5. Anticoagulant treatment was continued in this case. One postoperative patient developed a minor peripheral thrombophlebitis during Sintrom therapy when his clotting time was 111/2 minutes. PTR was 48%. Recovery from this episode was complete after five days of more adequate Sintrom therapy. Two patients with acute myocardial infarction died during the course of therapy.
DISCUSSION In our study of the relationship between
On 125 treatment days when the PTR was between 10 and 20%yo, the SCT record was as follows: below 15 minutes, 31 days; 15-20 minutes, 66 days; 21-25 minutes, 23 days; and 26-30 minutes, 5 days. On 56 treatment days when the PTR was under 10%, the SCT readings were as follows: less than 15 minutes, 13 days; 15-20 minutes, 27 days; 21-25 minutes, 14 days; 26-30 minutes, 1 day; and over 31 minutes, 1 day.
TABLE V.-SCT
SCT ranges Less than 15'..... 15 - 20'........... 21 - 25' ........... 26 - 30 .......... 31'and over. Total .......
AND
PTR RANGES WHEN SINTROM WAS
Treatment days No. % 271 38% 130 18% 138 19% 125 17%
THE SOLE ANTICOAGULANT
No.
Treatment days PTR range8 % 106 15% 41 and above. 509 71% 31- 40% ......... 89 12% 21 - 30% ......... 15 2%10 - 20% ......... 1 Less than 10%.. Total ........ 720 100%
56 720
8% 100%
The statistical analysis of daily Sintrom dosage is shown in Table VI.
oral anticoagulants and standardized clotting time we have been particularly interested in comparing the effects of Sintrom with those previously noted during dicoumarol therapy. In the present study anticoagulant therapy was directed solely by SCT readings, while in the previous investigation, PTR values were used to control therapy. In the current study we found, as we had with dicoumarol, that adequate doses of Sintrom produced significant SCT prolongation in all cases. Judged by the SCT, the time required to produce a satisfactory therapeutic value of 15 minutes was similar with the two drugs-4.3 days with Sintrom (Table III), 4.9 days with dicoumarol. A PTR value of 30% was obtained in the dicoumarol series in an average time of 3.15 days, and in Sintrom series in 2.2 days (Table IV). The relatively rapid PTR reduction with Sintrom has been accepted by other workers as proof that Sintrom has a more rapid anticoagulant effect than has dicoumarol. Our data, however, demonstrate no significant difference in the speed of onset of effective action of these two drugs, as judged
276 MAYER AND CONNELL: SINTROM
TABLE VI.-AVERAGE DAILY DosEs OF SINTROM IN MG. DURING THE FIRST 20 DAYs oF TREATMENT
Days of
Canad. M. A. J. Feb. 15,1957, vol. 76
treatment
|3
42
12.57
4
40
10.20
7
39
7.0
8 34
6.76
9
34
5.52
10
33
5.12
11 31
5.93
12
32
5.59
13
29
5.51
14
28
5.28
15
27
5.59
16
17
18
26
5.3
19 22
5.18
n..
... ..
42
22.57
42
17.42
41
8.24
41
7.60
28
5.42
26
5.5
21
4.71
Mean arithmetic..
.*2.90*1 2.46 *A 2.57 *3.02 *3.66 3.63 3.73 3.59 *3.03 2.82 3.04 *2.58 2.57 2.2 *3.0 *4-2.74 2.56 2.48 2.61 *L-2.6 SD .*.44*0.37 *0.39 *0.47 *9.57 *0.56 *0.59 *0.61 *0.57 *0.39 *0.54 *0.45 *0.47 *0.41 *0.57 *0.51 *0.5 *L-0.48 *0.55 *0.58 SE
by their effect on the clotting tendency of whole blood in vitro. The practical implication'is that patients on Sintrom therapy require heparin during the first four to five treatmnent days, if thrombo-embolism is to be avoided during this important period. One point of difference from dicoumarol should be stressed. Tables I and II demonstrate that a steady rise of the SCT to the therapeutic level of 15 minutes was achieved only by doses of Sintrom that depressed markedly the PTR. With dicoumarol, we seldom found such marked PTR depression associated with merely adequate SCT levels, early in the therapy. After the first eight days of Sintrom therapy, the mean PTR values approximated those of the dicoumarol series. However, with equivalent PTR readings, the SCT was significantly lower than in dicoumarol study. In other words, therapeutically adequate SCT levels during Sintrom administration were associated with more marked PTR depression than during dicoumarol therapy. This may represent a difference in the biological action of the two drugs. The anticoagulant effect (gauged by SCT and PTR) of Sintrom subsided completely in two or three days after cessation of therapy. This is significantly shorter than that we found with dicoumarol (six to seven days). In the evaluation of the SCT method in the control of Sintrom therapy it was important to investigate the relationship between SCT and PTR readings. Simple inspection of the individual curves showed some correlation: whenever PTR in per cent decreased, the SCT reading increased. However, this correlation was found to be only a qualitative one. The correlation coefficients varied from -0.1 to -0.47, that is from a poor to an approximate correlation. Further statistical calculation using Bernstein and Weatherall" criteria showed that the correlation coefficients did not significantly differ from zero; in other words, there was no quantitative correlation betw-een the two 'tests. A very similar result was obtained in our dic6umarol study.'
Table V shows that SCT was within our arbitrary therapeutic range on 71% of treatment days. On 15%o of the treatment days there was "undertreatment" and on 14% "overtreatment". Simultaneous PTR readings varied widely, being most of the time above the generally accepted therapeutic limits. If judged by the PTR values obtained during this study, the anticoagulant therapy should have been "poor". Actually, our clinical results were excellent, with only one minor bleeding and one small thrombophlebitis. In both cases SCT readings gave clear warning of danger, while PTR did not. In our previous study on dicoumarol' we tried to keep the PTR between 20 and 30%generally considered as the safe therapeutic range. This aim was achieved on only 36% of treatment days, which is comparable to other reports in the literature.9 A comparison of the therapeutically adequate SCT readings in the Sintrom series (71 % of treatment days) with the generally accepted safe PTR values in the dicoumarol series (36% of treatment days) shows clearly that' it is easier to maintain therapeutically desirable SCT values than currently acceptable PTR readings. It will be remarked that on 106 treatment days SCT values of less than 15 minutes were recorded, most of these in the early part of our study. They followed the omission or too great reduction of Sintrom on the day after an excessively high SCT reading. As our study progressed, we learned to anticipate these excessive drops, and to avoid them by more cautious reduction of dosage. Otherwise, if the drug'is omitted even for a day, the SCT may return near to the starting value, and is often not restored to an adequate therapeutic range until a further three or four days of treatment have been given.' Why had we only one thromboembolic episode during 106 treatment days
*Some difficulty was encountered in adjusting the daily maintenance doses, due to the fact that Sintrom was available to us only in 4-mg. tablets. From our experience, we feel that tablets containing 1 mg. of the active ingredient (besides 4-mg. tablets) are necessary to permit accurate adjustment of maintenance doses.
Canad. M. A. J. Canad. Feb. 15, 1957, vol. 76 VOl.
76
M. A. J.
~~~~MAYER AND CONNELL: SINTROM 277 MYRAD~NEL ITO a
guidance than do the Quick one-stage prothrombin readings.
SUMMARY 1. Forty-two patients have been studied during anticoagulant therapy with Sintrom (Geigy) for a period of 866 treatment days, control being maintained with the standardized clotting time
when the clotting time was under 15 minutes? Actually, on 67 of these days the SCT was 14 minutes, which is within the fiducial limits of 15 minutes. However, on 29 days it was 13 minutes, and on 10 days, less than this. Probably our lower therapeutic limit should be less than 15 minutes. We would point to the brilliant studies of Wesslerl who showed that, in addition to biological changes in the blood clotting mechanism, local factors play an important role in thrombus formation. Local factors promoting thrombosis were no doubt absent in those patients who did not develop thrombosis despite SCT readings which we consider too low. The single thrombotic episode we report does give clear warning that for proper handling of anticoagulant therapy, control must indeed be meticulous. We have now developed great confidence in our test. We would avoid in future routine therapy excessive rises of SCT such as were permitted to occur during this study-that is, readings of 21 to 25 minutes on 89 treatment days, and of between 26 and 30 minutes on 15 treatment days (Table V). We encountered only one minor bleeding during 105 days when the SCT was more than 20 minutes. This is much better than our experience during the previous dicoumarol series, when we had eight bleedings during 166 treatment days when the SCT was similarly elevated above 20 minutes. There are several reasons for this relative freedom from haemorrhage. 1. When dicoumarol was given and the SCT rose too high, it often remained elevated for several days in spite of the reduction or omission of drug, and most of our bleedings occurred after two or three days of excessive SCT readings. With Sintrom, we rarely saw a high reading for two consecutive days because the reduction of dose was followed by a rapid drop in SCT. 2. The pharmacological differences in the two drugs may of course be important in this respect. 3. Finally, there is the fact that in the dicoumarol study the Quick one-stage prothrombin test was used as the control, while in the current study, treatment was regulated entirely by- the standardized clotting time. This, we feel, is the major reason for our improved therapeutic record. Our present study indicates that in the clinical management of Sintrom therapy, as with dicoumarol,1 the SCT values provide more reliable
(SCT).
2. Sintrom produced a therapeutic prolongation of the SCT (15 minutes) after an average induction period of 4.3 days. 3. No haemorrhagic accidents or thromboembolic complications were noted when the SCT was maintained within our therapeutic range. 4. When Sintrom therapy was discontinued, the SCT returned to its pre-treatment level in from 48 to 72 hours. 5. Under the conditions of this study, Sintrom proved to be a satisfactory oral anticoagplant for short-term therapy. 6. Sintrom therapy was adequately and easily controlled by the standardized clotting time. 7. No significant correlation was found between the Quick one-stage prothrombin test and the standardized clotting time.
We wish to thank Miss Gwendolyn D. Thorp, R.N., for her valuable assistance and help.
REFERENCES 1. MAYER, G. A. AND CONNELL, W. F.: J. A. M. A., 161: 806, 1956. 2. STOLL, W. G. AND LITVAN, F.: In, International Conference on Thrombosis and Embolism, I, Basel, 1954, edited by T. Koller and W. R. Merz, Benno Schwabe and Co., Basel, 1955, p. 244. 3. WEINER, M., JIMINEZ, M. AND KATZKA, I.: Circulation, 13: 400, 1956. 4. MONTIGEL, C. AND PIJLVER, R.: In, International Conference on Thrombosis and Embolism, I, Basel, 1954, edited by T. Koller and W. R. Merz, Benno Schwabe and Co., Basel, 1955, p. 250. 5. BEAUMONT, J. L.: Ibid., p. 259. 6. AEPPLI, H. AND RUBELI, P.: Ibid., p. 265. 7. MAYER, G. A.: Canad. M. A. J., 72: 927, 1955.
9. WRIGHT, I. S., MARPLE, C. D. AND BEcK, D. F.: Myocardial infarction, its clinical manifestations and treatment with anticoagulants, Grune & Stratton, Inc., New York, 1954, p. 354. 10. WESSLER, S.: J. Clin. Invest., 34: 647, 1955. 11. BERNSTEIN, L. AND WEATHERALL, M.: Statistics for medical and other biological students, E. & S. Livingstone, Ltd., Edinburgh and London, 1952.
8. QUICK, A. J.: J. A. M. A., 110: 1658, 1938.
RESUME
Pendant la dur6e globale de 885 jours au cours desquels 42 malades furent soumis a une th6erapeutique anticoagulante basee sur le "Sintrom" (marque d6 m6e), on obtint un prolongement constant du temps e coagulation du sang frais. Ce medicament donna son plein rendement dans une moyenne de 4.3 jours apres la dose initiale (20 a 24 mg.), en quoi il est comparable a la dicoumarine. II est done important, si l'on d6sire retarder d'emblee le mecanisme de la coagulation, d'administrer de l'heparine au cours des deux ou trois premiers jours du traitement.
278 BAIN AND
OTHERS:
GALACrosMuA
Canad. Feb. 15,M. A. J. 76 1957, vol.
L'action du "Sintrom" est assez breve, disparaissant dans les 48 a 72 heures qui suivent l'arret e. la therapie. Aucune complication hemorragique ou thromboembolique ne survint pendant son emploi, et le temps de coagulation fut presque toujours maintenu dans les limites que l'on accepte comme valables en therapeutique. Les auteurs en ont dirige 1'administration d'apres les resultats du temps de coagulation d6termine par une
m6thode decrite anterieurement et standardisee selon des techniques maintenues rigoureusement identiques. Mayer et Connell semblent convaincus de la sup6riorit6 de cette methode par rapport a la m6thode en un temps de Quick pour la determination du temps de prothrombine. Ils n'ont d'ailleurs obtenu aucune corr6lation quantitative entre les deux genres de determination. D'apres eux, le "Sintrom" se classerait comme un anticoagulant oral satisfaisant dans les traitements a courte echeance. M.R.D.
GALACTOSAEMIA*
HARRY W. BAIN, M.D., DRUMMOND H. BOWDEN, M.D., A. LAWRENCE CHUTE, M.D., SANFORD H. JACKSON, M.D., ANDREW SASS-KORTSAK, M.D. and NORMA FORD WALKER, M.D., Toronto
GALACTOSAEMIA - COMMONER THAN WE THINK?
GALACTOSA,MIA or galactose diabetes is a congenital familial inborn error of metabolism characterized by an inability to metabolize lactose and galactose normally. To the infant this is a major catastrophe since his diet consists almost entirely of milk - the only important source of these substances. The essential features of the resulting syndrome are: severe malnutrition, hepatomegaly and the presence of a reducing substance (galactose), often with albumin and casts, in the urine. Lamellar cataracts have been present in many of the reported cases when carefully searched for with a slit lamp. Mental retardation may occur. Jaundice is being reported in an increasingly large proportion of the cases, and failure to report it in others is probably due to the fact that it is confused with physiological icterus of the newborn. Various types of liver lesion have been recorded in autopsy cases. By simply removing milk from fhe diet of these affected infants, the entire process is halted or reversed, and a slowly or rapidly fatal illness becomes merely an inconvenience-the inconvenience of supplying a milk substitute.
REVIEW OF LiTERURE The syndrome was first described in 1908 by von Reuss.' Goppert2 in 1917 reported the
*From the Department of Pmediatrics, University of Toronto, and The Research Institute of the Hospital for Sick Children, Toronto, Canada.
familial nature of the condition. Little appeared in the literature until 1934 and 1935 when Unshelm3 and then Mason and Turner' reported cases. Norman and Fashena5 added a case in 1948, as did Mellinkoff6 and his colleagues in 1945. Bruck and Rapoport,7 also in 1945, reported a case in a seven-week-old infant and suggested that the various manifestations were due to a direct toxic effect of galactose on the tissues. Goldbloom and Brickman8 reported two cases in 1946, with observations on the effect of insulin. Goldstein and Ennis9 in 1948 reported a case with abnormal liver function tests. In the same year, Greenman and Rathbunlo demonstrated improvement in galactose tolerance (as evidenced by intravenous galactose administration) by administering insulin and/or glucose, and advised the use of a high carbohydrate diet. Bell et al.1" 12 in 1950 reported two affected sibs, with a discussion of pathological studies of the liver as well as liver function tests. Townsend, Mason and Strong13 in 1951 added five additional cases and postulated a relationship of the liver changes to Laennec's cirrhosis. They presented also a 10-year follow-up on the case reported by Mason and Turner. In the same year, Donnell and Lann14 reported four cases, with comments on pathology and genetic aspects. Bray, Isaac and Watkins"5 in 1952 presented three cases from "the English literature, with observations on liver pathology and urine amino acid studies. One purpose of the present paper is to suggest that galactosaemia is, in reality, relatively common, and that the diagnosis is missed for several very good reasons: (1) Failure to obtain a urine specimen while the infant is on a milk feeding. (2) Failure to consider the diagnosis in all dystrophic and marasmic infants.
Vous aimerez peut-être aussi
- Grille Management Gps STDocument16 pagesGrille Management Gps STfidel AGUIDISSOUPas encore d'évaluation
- Acupuncture TraditionnelleDocument6 pagesAcupuncture Traditionnellejihem MottePas encore d'évaluation
- Guide Traitement Pharmacologique TDAHDocument1 pageGuide Traitement Pharmacologique TDAHsara harvey vachonPas encore d'évaluation
- Med 5an16 Rhumato SpondylarthritesDocument76 pagesMed 5an16 Rhumato Spondylarthritesimene BahriPas encore d'évaluation
- David Frawley - La Santé Par L'ayurvéda PDFDocument271 pagesDavid Frawley - La Santé Par L'ayurvéda PDFSimon Hacheme100% (2)
- Imagerie Des Tumeurs Malignes Primitives BronchopumonairesDocument18 pagesImagerie Des Tumeurs Malignes Primitives BronchopumonairesGhost ProPas encore d'évaluation
- PROJET AnimationDocument9 pagesPROJET AnimationInès 28Pas encore d'évaluation
- Cours Suivi PostnatalDocument35 pagesCours Suivi PostnatalBerthe TchifamPas encore d'évaluation
- Strategie AsthmeDocument13 pagesStrategie AsthmeEliezer YoungPas encore d'évaluation
- Note Explicative Titre de Séjour SantéDocument2 pagesNote Explicative Titre de Séjour Santérautierp6Pas encore d'évaluation
- Gestion de SaludDocument1 pageGestion de Saluddavidvilla0104Pas encore d'évaluation
- La CommunicationDocument36 pagesLa CommunicationrachidPas encore d'évaluation
- Hyper Prolactin EmieDocument24 pagesHyper Prolactin EmieWalid MesliPas encore d'évaluation
- Questionnaire PersonnaliséDocument7 pagesQuestionnaire PersonnaliséOmar DriraPas encore d'évaluation
- Toxocarose 1 3em 12Document6 pagesToxocarose 1 3em 12MACON824Pas encore d'évaluation
- Staphylococcus InfectionDocument19 pagesStaphylococcus InfectionImane AbPas encore d'évaluation
- Module 8 Champs D Applications Du Magne Tisme Les Maladies PhysiquesDocument61 pagesModule 8 Champs D Applications Du Magne Tisme Les Maladies PhysiquesnathaliebariselePas encore d'évaluation
- Module 02 - Réglementation SécuritéDocument39 pagesModule 02 - Réglementation SécuritéTarik GhassPas encore d'évaluation
- Abrege-Hge-Cd - 2015 - Chap29 - Item302 - Ue9 - Tumeurs de L'oesophageDocument9 pagesAbrege-Hge-Cd - 2015 - Chap29 - Item302 - Ue9 - Tumeurs de L'oesophagewooden latexPas encore d'évaluation
- Remerciement 2Document12 pagesRemerciement 2Ikram MecPas encore d'évaluation
- سمات الشخصية لدى المرضى السيكوسوماتيينDocument12 pagesسمات الشخصية لدى المرضى السيكوسوماتيينHouda NourPas encore d'évaluation
- Hamer Ryke Geerd - Le SIDA PDFDocument50 pagesHamer Ryke Geerd - Le SIDA PDFbidon50Pas encore d'évaluation
- Examen Clinique 2012Document54 pagesExamen Clinique 2012nidartsPas encore d'évaluation
- Crise - D'asthme Prise en Charge PDFDocument0 pageCrise - D'asthme Prise en Charge PDFjuniorebindaPas encore d'évaluation
- 10.la SplénomégalieDocument32 pages10.la Splénomégalieyves100% (1)
- 1.1.13ecrit Cours ThrombosesDocument11 pages1.1.13ecrit Cours Thrombosesmalick SemourPas encore d'évaluation
- 06 Financement Systeme Sante ChaoucheDocument13 pages06 Financement Systeme Sante ChaouchedrissechoPas encore d'évaluation
- Recette Naturelle Contre La VaricocèleDocument5 pagesRecette Naturelle Contre La VaricocèleCedricPas encore d'évaluation
- Liste Des 400 Médicaments Cancérigènes 2014Document20 pagesListe Des 400 Médicaments Cancérigènes 2014Maxime GardesPas encore d'évaluation
- Enoncé QCU TBL1 17sep2021Document24 pagesEnoncé QCU TBL1 17sep2021Azza LakhalPas encore d'évaluation