Vous aimerez peut-être aussi
- Performance et nutrition sportive: Guide pratique des facteurs nutritionnels qui influencent la performance physiqueD'EverandPerformance et nutrition sportive: Guide pratique des facteurs nutritionnels qui influencent la performance physiqueÉvaluation : 2 sur 5 étoiles2/5 (1)
- Artigo 12 JFDocument6 pagesArtigo 12 JFJailson CamposPas encore d'évaluation
- Rhu.0b013e318190f95f FRDocument12 pagesRhu.0b013e318190f95f FRdidikhadija2022Pas encore d'évaluation
- Frankwein@yahoo - FR: Abstracts / Revue de Chirurgie Orthopédique Et Traumatologique 104 (2018) S68-S111 S75Document1 pageFrankwein@yahoo - FR: Abstracts / Revue de Chirurgie Orthopédique Et Traumatologique 104 (2018) S68-S111 S75oliv starPas encore d'évaluation
- La Kinesitherapie Analytique - Thérapie Manuelle Selon Le Concept Sohier PrésentationDocument5 pagesLa Kinesitherapie Analytique - Thérapie Manuelle Selon Le Concept Sohier PrésentationAnāïssę Mk100% (1)
- Rééducation Cheville Et Pied ProprioceptionDocument3 pagesRééducation Cheville Et Pied ProprioceptionCathy ToyaPas encore d'évaluation
- Lederman - La Chute Du Model Postural Structurel BiomecaniqueDocument16 pagesLederman - La Chute Du Model Postural Structurel BiomecaniqueJulien LovadinaPas encore d'évaluation
- Orthopedie Polycopie PR Lerat 09 Systeme MusculaireDocument35 pagesOrthopedie Polycopie PR Lerat 09 Systeme MusculaireBodeanu Suzana MihaelsPas encore d'évaluation
- PEC Épaule: ACDocument17 pagesPEC Épaule: ACGaelle BaudequinPas encore d'évaluation
- 10 1016@j Kine 2016 07 001 PDFDocument2 pages10 1016@j Kine 2016 07 001 PDFMjidKarimPas encore d'évaluation
- Facilitation Proprioceptive Neuromusculaire (PNF) Kiné Actualité PDFDocument4 pagesFacilitation Proprioceptive Neuromusculaire (PNF) Kiné Actualité PDFOussama Kherdi100% (1)
- TBSc2020 Isidoro Oliveira Ranzoni SharaihaDocument68 pagesTBSc2020 Isidoro Oliveira Ranzoni Sharaihaerwan.gir26Pas encore d'évaluation
- Posturologie Posturopodie PodologueDocument2 pagesPosturologie Posturopodie PodologueZund AlphaPas encore d'évaluation
- Bilan MorphostatiqueDocument69 pagesBilan MorphostatiqueJedidi Amir50% (4)
- Effet Manipulations Vertébrale Dans La Prise en Charge ChroniqueDocument320 pagesEffet Manipulations Vertébrale Dans La Prise en Charge ChroniqueCloé SzcPas encore d'évaluation
- Rééducation LombalgiquesDocument10 pagesRééducation Lombalgiquesbenben31100% (1)
- Effets Des Postures de Relâchement Selon La Méthode BusquetDocument8 pagesEffets Des Postures de Relâchement Selon La Méthode BusquetAmï NãPas encore d'évaluation
- J Nupar 2009 10 010Document6 pagesJ Nupar 2009 10 010Oum BanatPas encore d'évaluation
- Fonction Articulaire Et Fonction Musculaire DR LAIBDocument8 pagesFonction Articulaire Et Fonction Musculaire DR LAIBRim BenguenabPas encore d'évaluation
- Mémoire DUP Compression in Athletes - From Concept To Reality. Effects of Compression Garments On Athletic Performance and Recovery Effort PDFDocument12 pagesMémoire DUP Compression in Athletes - From Concept To Reality. Effects of Compression Garments On Athletic Performance and Recovery Effort PDFCoach-NeilKhayechPas encore d'évaluation
- Berck 2007 BURDIN LigamentoplastieDocument38 pagesBerck 2007 BURDIN LigamentoplastieMarius PopescuPas encore d'évaluation
- Travail de Session KIN 708Document13 pagesTravail de Session KIN 708Rebecca BeaudettePas encore d'évaluation
- 2002 Entorsecheville EMCDocument26 pages2002 Entorsecheville EMCNouha ChellaliPas encore d'évaluation
- Le Bilan Et Le Diagnostic Kinésithérapique: G. PéninouDocument12 pagesLe Bilan Et Le Diagnostic Kinésithérapique: G. PéninouŘīă WivgelrePas encore d'évaluation
- Kdoc PDFDocument44 pagesKdoc PDFNada GhammemPas encore d'évaluation
- 12 Physiopathologie HagerDocument26 pages12 Physiopathologie HagerTikouk TaoufikPas encore d'évaluation
- 2012 PDFLMPRVestibulaireDocument7 pages2012 PDFLMPRVestibulairekarim.acpePas encore d'évaluation
- Biologie 5 SecondaireDocument13 pagesBiologie 5 SecondaireJean Claude ImenedipyPas encore d'évaluation
- SYndrome RotulienDocument3 pagesSYndrome RotulienobisoPas encore d'évaluation
- Muscles ProfondsDocument89 pagesMuscles Profondsceline salsaPas encore d'évaluation
- Spasticite, Douleur Et Toxine BotuliniqueDocument4 pagesSpasticite, Douleur Et Toxine BotuliniqueAicha BenzagoutaPas encore d'évaluation
- Toxine BotuliqueeDocument4 pagesToxine BotuliqueeAicha BenzagoutaPas encore d'évaluation
- RTS & RTC Post Ligamentoplastie LCADocument5 pagesRTS & RTC Post Ligamentoplastie LCAMedPas encore d'évaluation
- ML 2 2013 71Document8 pagesML 2 2013 71sanijikram11Pas encore d'évaluation
- Proprioception Du Rachis Cervical - Une Approche ActualiséeDocument8 pagesProprioception Du Rachis Cervical - Une Approche ActualiséearbedPas encore d'évaluation
- Reeducation Uro-Gynecologique Feminine TechniquesDocument12 pagesReeducation Uro-Gynecologique Feminine TechniquesAquarelle Prothesiste OngulairePas encore d'évaluation
- Cervicalgie TT ManuelDocument7 pagesCervicalgie TT ManuelGaelle BaudequinPas encore d'évaluation
- Reeducation Hanche OpéréDocument32 pagesReeducation Hanche OpéréJedidi AmirPas encore d'évaluation
- 06-Syndrome Fémoropatellaire - Prise en Charge CliniqueDocument11 pages06-Syndrome Fémoropatellaire - Prise en Charge CliniqueMayssa Ould kaciPas encore d'évaluation
- News 09Document7 pagesNews 09Sebastien Van ImpePas encore d'évaluation
- Anatfonct PSM2Document81 pagesAnatfonct PSM2ratzilla187Pas encore d'évaluation
- Pau TorontoDocument20 pagesPau TorontobonjourPas encore d'évaluation
- Semiologie HancheDocument20 pagesSemiologie HancheCrn HmdPas encore d'évaluation
- News 08Document7 pagesNews 08Sebastien Van ImpePas encore d'évaluation
- Technique de McKenzie Dans La LombalgieDocument12 pagesTechnique de McKenzie Dans La LombalgieJedidi AmirPas encore d'évaluation
- Catalogue OIA 2023Document20 pagesCatalogue OIA 2023malikPas encore d'évaluation
- Le Concept Sohier: Application À L'articulation Coxo-FémoraleDocument9 pagesLe Concept Sohier: Application À L'articulation Coxo-FémoralemitroisergiuPas encore d'évaluation
- Bilan MusculaireDocument5 pagesBilan MusculairenaoPas encore d'évaluation
- Examen NeurologiqueDocument11 pagesExamen NeurologiqueHoussemPas encore d'évaluation
- Cours Illustré PLANDocument15 pagesCours Illustré PLANalexkinePas encore d'évaluation
- 76 5 Vautravers PDFDocument5 pages76 5 Vautravers PDFnirvadinePas encore d'évaluation
- Brismee-Hydratation Discale-2023-11-20Document22 pagesBrismee-Hydratation Discale-2023-11-20Rhim MohamedPas encore d'évaluation
- Résultats de La Rééducation de L'incontinence Urinaire de L'homme Après Chirurgie ProstatiqueDocument8 pagesRésultats de La Rééducation de L'incontinence Urinaire de L'homme Après Chirurgie ProstatiqueHALIFAPas encore d'évaluation
- Article Scientifique Hapo Ms - FRDocument10 pagesArticle Scientifique Hapo Ms - FRghalem bennailaPas encore d'évaluation
- Cours de Kinesitherapie Eide IiiDocument19 pagesCours de Kinesitherapie Eide Iiideliephrahim835Pas encore d'évaluation
- Présentation Cours 1 Helha 2Document56 pagesPrésentation Cours 1 Helha 2vzc7974pxfPas encore d'évaluation
- SouplesseDocument25 pagesSouplesseJulien MunozPas encore d'évaluation
- Therapiemanuellepied PDFDocument16 pagesTherapiemanuellepied PDFMjidKarim100% (1)
- Lésiosn Scapulaires de Surcharge Et Sports de LancerDocument6 pagesLésiosn Scapulaires de Surcharge Et Sports de Lancermae.bsd2001Pas encore d'évaluation
- Biochimie Du LCRDocument7 pagesBiochimie Du LCRnesrine27029Pas encore d'évaluation
- Dysfonction de L'appareil Manducateur: 2-RééducationDocument4 pagesDysfonction de L'appareil Manducateur: 2-RééducationSaadia BensadokPas encore d'évaluation
- Laryngites Chroniques: L. Plisson, P. Demez, C. Dolfus, E. Lechapt, M. Hitier, E. BabinDocument16 pagesLaryngites Chroniques: L. Plisson, P. Demez, C. Dolfus, E. Lechapt, M. Hitier, E. BabinMoncef Pecha100% (1)
- I) Evaluation Des Resssources Partie A: Evaluation Des Savoirs Exercice 1: Questions À Choix Multiples (QCM)Document8 pagesI) Evaluation Des Resssources Partie A: Evaluation Des Savoirs Exercice 1: Questions À Choix Multiples (QCM)mahopfranck092Pas encore d'évaluation
- C31. Appareil Génital FémininDocument10 pagesC31. Appareil Génital Fémininnacim fethy halesPas encore d'évaluation
- 04 Ostéologie de La JambeDocument7 pages04 Ostéologie de La Jambeeladib p1Pas encore d'évaluation
- Genetique Fiche BrevetDocument2 pagesGenetique Fiche BrevetdrissPas encore d'évaluation
- Communication Inter-CellulaireDocument48 pagesCommunication Inter-CellulaireMahmoud Abbas El'Andaloussi BenbrahimPas encore d'évaluation
- Les Ovaires. DR BaDocument7 pagesLes Ovaires. DR BaAbdoul karim SamakePas encore d'évaluation
- Leçon SVT GénétiqueDocument9 pagesLeçon SVT GénétiqueKairozZ FPSPas encore d'évaluation
- Coeur Anatomie 3Document62 pagesCoeur Anatomie 3Aek BenguerrahPas encore d'évaluation
- Affections Du CPD, 2è A...Document57 pagesAffections Du CPD, 2è A...landry kendryPas encore d'évaluation
- 34 Plaquettes SanguinesDocument8 pages34 Plaquettes SanguinesmaryPas encore d'évaluation
- Résumétransmission de IG Complet Méiose Fecondation 15.Document2 pagesRésumétransmission de IG Complet Méiose Fecondation 15.youssefbanqPas encore d'évaluation
- La Megacaryopoïese.Document1 pageLa Megacaryopoïese.Najwa MansourPas encore d'évaluation
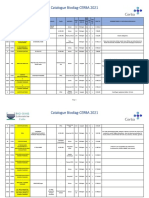
- Catalogue Biodiag-CERBA 2021Document179 pagesCatalogue Biodiag-CERBA 2021Halima BgrPas encore d'évaluation
- Anomalies de Signal IRM Substance Blanche CérébraleDocument11 pagesAnomalies de Signal IRM Substance Blanche CérébraleSoumia El ArabiPas encore d'évaluation
- Kos Wolf MenisquesDocument11 pagesKos Wolf MenisquesfilorpgPas encore d'évaluation
- Lcet 'Document31 pagesLcet 'mehdi hatimPas encore d'évaluation
- Coxo-Fém FZ PDFDocument8 pagesCoxo-Fém FZ PDFFirdaws BentenniPas encore d'évaluation
- Correction Série 1 Annexe Reproduction Masculine Partie 1Document3 pagesCorrection Série 1 Annexe Reproduction Masculine Partie 1KhawlaPas encore d'évaluation
- Os TemporalDocument25 pagesOs TemporalvendezioPas encore d'évaluation
- Physiologie Digestive 2021 ÉtudiantsDocument12 pagesPhysiologie Digestive 2021 ÉtudiantsomarmoustaqPas encore d'évaluation
- Physiologie FCT MusculaireDocument14 pagesPhysiologie FCT MusculaireJon FuagaPas encore d'évaluation
- Physiologie de L'oesophage - Mon Cours Jan 2015Document11 pagesPhysiologie de L'oesophage - Mon Cours Jan 2015Merou Koubi100% (2)
- Le FoieDocument153 pagesLe FoieHicham ZiyaniPas encore d'évaluation
- Hemato SDQ2307-1041Document1 pageHemato SDQ2307-1041Hassan ZahidiPas encore d'évaluation
- Exercices Corriges Le Soi Et Le Non Soi Les BasesDocument5 pagesExercices Corriges Le Soi Et Le Non Soi Les BasesChristian abahPas encore d'évaluation
- I) Effet DopplerDocument3 pagesI) Effet DopplerjonadasmathieuPas encore d'évaluation
- Etude D'un'effecteur Moteur Le Muscle Strié SquelettiqueDocument6 pagesEtude D'un'effecteur Moteur Le Muscle Strié SquelettiqueBathie SarrPas encore d'évaluation