Vous aimerez peut-être aussi
- Évaluation Des Risque ProfessionnelsDocument12 pagesÉvaluation Des Risque ProfessionnelsAngelicaBarry100% (1)
- L AppendiciteDocument3 pagesL AppendiciteKhaoulaFaithful100% (2)
- Urg de Garde CAT ProtocolesDocument186 pagesUrg de Garde CAT ProtocolesBA MBENEPas encore d'évaluation
- Premiers Secours: un manuel pratique pour faire face aux urgencesD'EverandPremiers Secours: un manuel pratique pour faire face aux urgencesPas encore d'évaluation
- Protocoles PediatriquesDocument88 pagesProtocoles PediatriquesFrancisPas encore d'évaluation
- Bronchiolite Fiche Technique 19 Mars 2020 PR RadouiDocument4 pagesBronchiolite Fiche Technique 19 Mars 2020 PR RadouibokolaPas encore d'évaluation
- Gastro31-Cholecystite Aigue LithiasiqueDocument3 pagesGastro31-Cholecystite Aigue LithiasiqueChichar LioPas encore d'évaluation
- La Médecine Traditionnelle Chinoise: Je Me SoigneDocument27 pagesLa Médecine Traditionnelle Chinoise: Je Me SoigneCrHésse Vèrmouth100% (1)
- Examen N.né CorrigéDocument72 pagesExamen N.né CorrigéAbdo Boukharta100% (2)
- Semiologie de L'enfantDocument59 pagesSemiologie de L'enfantkamil09Pas encore d'évaluation
- Sémiologie Pédiatrique PDFDocument138 pagesSémiologie Pédiatrique PDFHéloïse MallaisyPas encore d'évaluation
- Introduction À La Toxicologie Des Médicaments KOULOUGHLI KhaoulaDocument29 pagesIntroduction À La Toxicologie Des Médicaments KOULOUGHLI KhaoulaKhaoola KLG0% (1)
- Bible PediatrieDocument88 pagesBible PediatrieIsrael Liwala100% (1)
- TP N - 1 - Observation en PediatrieDocument19 pagesTP N - 1 - Observation en Pediatrieanis anis50% (2)
- Cardio LogieDocument84 pagesCardio LogieBõuŤhęyÑãPas encore d'évaluation
- Pediatrie5an-Detresse Respiratoire Nn2020benhacineDocument8 pagesPediatrie5an-Detresse Respiratoire Nn2020benhacinedfsddPas encore d'évaluation
- Medecine ChinoiseDocument29 pagesMedecine Chinoisejonathan.boussoir22150% (1)
- Hypertension Arterielle Et GrossesseDocument6 pagesHypertension Arterielle Et Grossessenedjet malimPas encore d'évaluation
- Sutures Chirurgicales: Un Manuel Pratique sur les Nœuds Chirurgicaux et les Techniques de Suture Utilisées dans les Premiers Secours, la Chirurgie et la Médecine GénéraleD'EverandSutures Chirurgicales: Un Manuel Pratique sur les Nœuds Chirurgicaux et les Techniques de Suture Utilisées dans les Premiers Secours, la Chirurgie et la Médecine GénéraleÉvaluation : 1 sur 5 étoiles1/5 (1)
- Asphyxie NeonataleDocument5 pagesAsphyxie NeonataleOusmane SambouPas encore d'évaluation
- Staphylococcie Pleuropulmonaire de L'enfantDocument36 pagesStaphylococcie Pleuropulmonaire de L'enfantAwana DimitriPas encore d'évaluation
- Détresses Respiratoire Du Nouveau NéDocument13 pagesDétresses Respiratoire Du Nouveau NésarahPas encore d'évaluation
- Petit Guide Des Urgence Pédiatrique Pour Les MedecinsDocument75 pagesPetit Guide Des Urgence Pédiatrique Pour Les MedecinsTinhinane ZiaPas encore d'évaluation
- Plan de Discussion Nephro-1Document11 pagesPlan de Discussion Nephro-1de100% (4)
- Asthme Chronique PDFDocument7 pagesAsthme Chronique PDFBMA-medecine100% (1)
- Cat Neonat ModifiéDocument75 pagesCat Neonat ModifiéAbdelghani InousPas encore d'évaluation
- Plantes - Lorier 2011Document2 pagesPlantes - Lorier 2011L'araucariaPas encore d'évaluation
- PEDIATRIE CHU Blida 2 PDFDocument430 pagesPEDIATRIE CHU Blida 2 PDFcondé talla100% (7)
- Bible de PediatrieDocument140 pagesBible de PediatrieconstantsamboPas encore d'évaluation
- Examen Clinique Du Nouveau Né Removed 2Document11 pagesExamen Clinique Du Nouveau Né Removed 2Jojo DodPas encore d'évaluation
- UntitledDocument282 pagesUntitledThe Curious الفضوليPas encore d'évaluation
- 024 Grossesse Extra-UtérineDocument2 pages024 Grossesse Extra-UtérineAboubacar SomparePas encore d'évaluation
- Psychose InfantileDocument13 pagesPsychose Infantileilestunefois100% (1)
- Protocole Hopital Universitaire Justinien 1Document63 pagesProtocole Hopital Universitaire Justinien 1Peguy GeffrardPas encore d'évaluation
- Jury PediatrieDocument12 pagesJury PediatrieChrys DesozaPas encore d'évaluation
- Reanimation Pediatrique PDFDocument51 pagesReanimation Pediatrique PDFFateh Kessad100% (1)
- Stage PédiatrieDocument27 pagesStage PédiatriemrabetPas encore d'évaluation
- Maladies InfantilesDocument6 pagesMaladies InfantilesKouekam Gustave TientcheuPas encore d'évaluation
- Plan Observation PédiatriqueDocument7 pagesPlan Observation Pédiatriquehp pc100% (1)
- Cours de Neonatologie Modifie - 062137 - 045803Document40 pagesCours de Neonatologie Modifie - 062137 - 045803augustinnzaji23Pas encore d'évaluation
- Fiche Controle MonitorageDocument4 pagesFiche Controle MonitorageArial BioPas encore d'évaluation
- Q016 - LeucorrheesDocument3 pagesQ016 - LeucorrheesdeadbysunriseePas encore d'évaluation
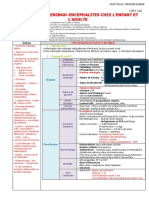
- 148 Méningites, Méningo-Encéphalites Chez L'enfant Et L'adulte - 0Document4 pages148 Méningites, Méningo-Encéphalites Chez L'enfant Et L'adulte - 0Amine KssiliPas encore d'évaluation
- Q 067 PancytopenieDocument4 pagesQ 067 PancytopenietoufikPas encore d'évaluation
- DG Masse Abd EnfantDocument28 pagesDG Masse Abd EnfantFlö Rã100% (1)
- Les Score de PediatrieDocument7 pagesLes Score de PediatriePierre KalalaPas encore d'évaluation
- Trousseau de Poche CompletDocument271 pagesTrousseau de Poche CompletfpguyaderPas encore d'évaluation
- Observation Médicale en PédiatrieDocument8 pagesObservation Médicale en PédiatrieKanezouné GongnetPas encore d'évaluation
- Tissemsilt Detresse Respiratoire Nouveau Ne AchourDocument34 pagesTissemsilt Detresse Respiratoire Nouveau Ne AchourMara NdiayePas encore d'évaluation
- Conduite À Tenir Devant Une Fièvre AigueDocument22 pagesConduite À Tenir Devant Une Fièvre AigueSerigne Sohibou Gaye100% (1)
- Detresse Respiratoire Du Nouveau Ne CHU Pellegrin-Bordeaux PDFDocument8 pagesDetresse Respiratoire Du Nouveau Ne CHU Pellegrin-Bordeaux PDFmoad ahmed100% (1)
- Examen Clinique Du Nné - Soins en Salle de NceDocument40 pagesExamen Clinique Du Nné - Soins en Salle de NceSerigne Sohibou GayePas encore d'évaluation
- L'Examen Clinique Du Nourrisson Et de L'enfantDocument39 pagesL'Examen Clinique Du Nourrisson Et de L'enfantFanny NicolasPas encore d'évaluation
- Asphyxie Néonatale ALIMADocument43 pagesAsphyxie Néonatale ALIMAFreddy CarelPas encore d'évaluation
- Conduite À Tenir Devant Une ProtéinurieDocument28 pagesConduite À Tenir Devant Une ProtéinurieStu DentPas encore d'évaluation
- Observations Cliniques CHU-B DR KAMISSOKO-1Document88 pagesObservations Cliniques CHU-B DR KAMISSOKO-1Souleymane GuiguemdePas encore d'évaluation
- La Prématurité.Document7 pagesLa Prématurité.anis anis100% (1)
- Les Grands SyndromesDocument61 pagesLes Grands Syndromeserwin NZOLPas encore d'évaluation
- Gina 2019Document40 pagesGina 2019حمود بوعلامPas encore d'évaluation
- CAT Sur Vomissements de L'enfantDocument28 pagesCAT Sur Vomissements de L'enfantSerigne Sohibou GayePas encore d'évaluation
- Urgences HypertensivesDocument42 pagesUrgences HypertensivesMohamed Mimou100% (1)
- Anémies Du Nouveau-NéDocument6 pagesAnémies Du Nouveau-NézerfaouiPas encore d'évaluation
- 159 CoquelucheDocument1 page159 CoquelucheAmine KssiliPas encore d'évaluation
- Copie de Ictère Nouveau-Né 2014Document96 pagesCopie de Ictère Nouveau-Né 2014Bouhannache MeryemPas encore d'évaluation
- Trousse D - 'Urgence en PédiatrieDocument3 pagesTrousse D - 'Urgence en PédiatrieAghiles Boussa100% (2)
- Deshydratation Aigue de L'enfantDocument21 pagesDeshydratation Aigue de L'enfantanis anisPas encore d'évaluation
- C22 - Cardiopathies CongénitalesDocument29 pagesC22 - Cardiopathies Congénitalesblue birdPas encore d'évaluation
- Chimie Environnementale Des Rejets UrbainsDocument5 pagesChimie Environnementale Des Rejets UrbainsAbdelhakim Bailal0% (1)
- Le Muscle SquelettiqueDocument4 pagesLe Muscle SquelettiqueGabriela TituPas encore d'évaluation
- Pathologie de L'œsophage Chez L'enfantDocument33 pagesPathologie de L'œsophage Chez L'enfantenimaPas encore d'évaluation
- MycologieDocument45 pagesMycologiesafemindPas encore d'évaluation
- Les Maladies de Dépérissement Des AgrumesDocument48 pagesLes Maladies de Dépérissement Des AgrumesMichelAndriamahazonoroRaherimanantsoaPas encore d'évaluation
- SPLANCHNOLOGIEDocument6 pagesSPLANCHNOLOGIEdhcbhvct7bPas encore d'évaluation
- Compte-Rendu 2Document2 pagesCompte-Rendu 2Ghislaine ViarougePas encore d'évaluation
- Speech BtsDocument6 pagesSpeech BtsStefen KenedyPas encore d'évaluation
- AntiarythmiquesDocument12 pagesAntiarythmiquesBarinaPas encore d'évaluation
- Cours 3Document177 pagesCours 3Christiane Elisa NGAFFOPas encore d'évaluation
- C'est Pas Sorcier DVD08c - Les MédicamentsDocument1 pageC'est Pas Sorcier DVD08c - Les MédicamentsBarbaraPas encore d'évaluation
- Correction Du Devoir C1 2011Document2 pagesCorrection Du Devoir C1 2011Mohamed SaidiPas encore d'évaluation
- Anticoagulants 2011Document53 pagesAnticoagulants 2011Abryda Ania AityPas encore d'évaluation
- Pieces Prise ChargeDocument11 pagesPieces Prise ChargeAhmed Hamid HamadPas encore d'évaluation
- Cah 7 Article 3Document6 pagesCah 7 Article 3pierre_ngPas encore d'évaluation
- Dhers Marcel-La CenestopathieDocument57 pagesDhers Marcel-La CenestopathieltbtawPas encore d'évaluation
- Neurologie II AVC PDFDocument10 pagesNeurologie II AVC PDFisiseaoPas encore d'évaluation
- FORMATIONSDocument3 pagesFORMATIONSMaurice MariotPas encore d'évaluation
- CV Antoine Capelle 2023Document1 pageCV Antoine Capelle 2023AntoineCapellePas encore d'évaluation
- Purpura Thrombopenique ImmunologiqueDocument74 pagesPurpura Thrombopenique ImmunologiqueHung HoangPas encore d'évaluation
- These29 13Document143 pagesThese29 13benhammadi najibPas encore d'évaluation