Vous aimerez peut-être aussi
- La Rythmologie Des JESFC 2022Document5 pagesLa Rythmologie Des JESFC 2022Ik RamPas encore d'évaluation
- Variabilité de La Fréquence CardiaqueDocument12 pagesVariabilité de La Fréquence CardiaqueDominique MellinPas encore d'évaluation
- 028+Koudougou+IC+Et+ANEMIE+Final+(1)Document5 pages028+Koudougou+IC+Et+ANEMIE+Final+(1)mutruc.victoria96Pas encore d'évaluation
- Choisir Avec Soin Collection of Lists PDFDocument146 pagesChoisir Avec Soin Collection of Lists PDFWellington BeneditoPas encore d'évaluation
- Choisir Avec Soin Collection of ListsDocument146 pagesChoisir Avec Soin Collection of ListsWellington BeneditoPas encore d'évaluation
- Linsuffisance CardiaqueDocument5 pagesLinsuffisance CardiaqueRamo BeckerPas encore d'évaluation
- 1HTA en Gériatrie Sept 2023 SyllDocument90 pages1HTA en Gériatrie Sept 2023 Syllmesut.saciPas encore d'évaluation
- MainDocument2 pagesMainhelmiensiPas encore d'évaluation
- 2014 RFE Choc-CardiogéniqueDocument10 pages2014 RFE Choc-CardiogéniqueSiv BibiPas encore d'évaluation
- Mlavillonniere,+lvrea 2018 Sprrea001275Document9 pagesMlavillonniere,+lvrea 2018 Sprrea001275Nada DnPas encore d'évaluation
- Dépistage Du Syndrome D'apnées Du Sommeil Par Le Cardiologue: de La Théorie À La PratiqueDocument5 pagesDépistage Du Syndrome D'apnées Du Sommeil Par Le Cardiologue: de La Théorie À La PratiqueSarah HouasniaPas encore d'évaluation
- 017+ao+akhaga+préopératoire+systématique+de+l'ecg+LBV (1)Document4 pages017+ao+akhaga+préopératoire+systématique+de+l'ecg+LBV (1)Kã MërPas encore d'évaluation
- Comment Évaluer Le Risque Hémorragique en Préopératoire - PDFDocument11 pagesComment Évaluer Le Risque Hémorragique en Préopératoire - PDFelaaPas encore d'évaluation
- LHTA Rsistante Journal Cardiologie PratiqueDocument3 pagesLHTA Rsistante Journal Cardiologie PratiqueRamo BeckerPas encore d'évaluation
- Hta PDFDocument65 pagesHta PDFMarc Randriatsarafara0% (1)
- Les Enquêtes ÉpidémiologiquesDocument23 pagesLes Enquêtes ÉpidémiologiquesMayssa BourenanePas encore d'évaluation
- Stress Testing After Complete RevaskDocument7 pagesStress Testing After Complete RevaskAstrid Karina PutriPas encore d'évaluation
- Avc PDFDocument87 pagesAvc PDFThiziri ThiziriPas encore d'évaluation
- Syndrome de Tako-TsuboDocument32 pagesSyndrome de Tako-Tsuboblk fatimaPas encore d'évaluation
- Insuffisance Cardiaque Memoire de Fatima2014Document33 pagesInsuffisance Cardiaque Memoire de Fatima2014Mehdi YahiPas encore d'évaluation
- Article Final TEMPO HCMDocument6 pagesArticle Final TEMPO HCMDalila Kazi TaniPas encore d'évaluation
- ProjetDocument18 pagesProjetmaryam.gynoPas encore d'évaluation
- 11 Grands Essais CardiovasculairesDocument9 pages11 Grands Essais CardiovasculairesDINO ECOPas encore d'évaluation
- Risque CVS LupusDocument7 pagesRisque CVS LupusHenry TraoréPas encore d'évaluation
- Syndrome D Apnee Obstructive Du Sommeil Et Anesthesie SAOS Jean-Francois PAYEN GrenobleDocument15 pagesSyndrome D Apnee Obstructive Du Sommeil Et Anesthesie SAOS Jean-Francois PAYEN Grenoblekarimsfar778Pas encore d'évaluation
- Protocole Publié Pr. Helmi Ben SAAD 2010-3Document9 pagesProtocole Publié Pr. Helmi Ben SAAD 2010-3Randaline AyoubPas encore d'évaluation
- Les Bêta-Bloquants en PratiqueDocument8 pagesLes Bêta-Bloquants en Pratiquemajdi ben salemPas encore d'évaluation
- Carot ManagDocument6 pagesCarot ManagKota AnuroopPas encore d'évaluation
- Knowledge, Attitudes and Practices of People Aged 60 Years and Older On Hypertension at The Ouakam Center For Gerontology and Geriatrics in 2018Document8 pagesKnowledge, Attitudes and Practices of People Aged 60 Years and Older On Hypertension at The Ouakam Center For Gerontology and Geriatrics in 2018hiba samlaliPas encore d'évaluation
- HTA DR BenyezzarDocument15 pagesHTA DR BenyezzarRaniaPas encore d'évaluation
- AVC Ischemique Nicolas BRUDER MarseilleDocument23 pagesAVC Ischemique Nicolas BRUDER MarseilleAvoksouma MichaelPas encore d'évaluation
- CAS CLINIQAUEJUIN 2014 Nouveau Document Microsoft Office Word - PDF FilenameDocument10 pagesCAS CLINIQAUEJUIN 2014 Nouveau Document Microsoft Office Word - PDF FilenameAnis Ali-khodjaPas encore d'évaluation
- Diagnostic Microbiologique Des Arthrites Septiques RMS 2019Document6 pagesDiagnostic Microbiologique Des Arthrites Septiques RMS 2019HoussemSoltanaPas encore d'évaluation
- Prévention Des Accidents Vasculaires CérébrauxDocument20 pagesPrévention Des Accidents Vasculaires CérébrauxaissaPas encore d'évaluation
- thrombophilie AVCDocument16 pagesthrombophilie AVCSFA_ANGEIOLOGIEPas encore d'évaluation
- 15h15scintigraphie Myocardique PDFDocument48 pages15h15scintigraphie Myocardique PDFYoucef ZianePas encore d'évaluation
- ExempleDocument12 pagesExempleIngrid KoutioPas encore d'évaluation
- Urgence - Re Animation: Le Smur Doit-Il Réanimer Tous Les Arrêts Cardiaques ?Document4 pagesUrgence - Re Animation: Le Smur Doit-Il Réanimer Tous Les Arrêts Cardiaques ?Myriam HadjarPas encore d'évaluation
- 07 Dysfonction Erectile Aspects Epidemiologiques Diagnostiques Et Therapeutiques AuDocument6 pages07 Dysfonction Erectile Aspects Epidemiologiques Diagnostiques Et Therapeutiques AuPaul OscarPas encore d'évaluation
- Coronarien Et AnesthésieDocument49 pagesCoronarien Et AnesthésielenkappartPas encore d'évaluation
- Hta 2Document49 pagesHta 2BMA-medecinePas encore d'évaluation
- Facteurs Pronostiques Du Cancer Du SeinDocument104 pagesFacteurs Pronostiques Du Cancer Du Seingiuseppe maldiPas encore d'évaluation
- Anesthesie - en - Chirurgie - Cardiaque-Sophie - Provenchere - 2005 2Document58 pagesAnesthesie - en - Chirurgie - Cardiaque-Sophie - Provenchere - 2005 2Harold PhilippotPas encore d'évaluation
- Quantification Et Traitement: Du Syndrome CongestifDocument5 pagesQuantification Et Traitement: Du Syndrome CongestifYouyouPas encore d'évaluation
- Recos CMH 2014Document6 pagesRecos CMH 2014Simona IonitaPas encore d'évaluation
- La Dysplasie Arythmogène Pertinence Des Examens DiagnostiquesDocument7 pagesLa Dysplasie Arythmogène Pertinence Des Examens DiagnostiquesAHOUANSOUPas encore d'évaluation
- 2019-04-Transfusion Patient Drépanocytaire FDocument1 page2019-04-Transfusion Patient Drépanocytaire FHerve MvoPas encore d'évaluation
- Place Du Bilan Dhemostase en Preoperatoire: Etude Des Pratiques de Lhopital Universitaire Jra Antananarivo MadagascarDocument8 pagesPlace Du Bilan Dhemostase en Preoperatoire: Etude Des Pratiques de Lhopital Universitaire Jra Antananarivo MadagascarIJAR JOURNALPas encore d'évaluation
- Consultation Anesthesie CoursDocument6 pagesConsultation Anesthesie CoursJustine DelattrePas encore d'évaluation
- Cardioscopies N 75 - 2000 PDFDocument21 pagesCardioscopies N 75 - 2000 PDFHuplala HypocratePas encore d'évaluation
- Fibrillation Auriculaire Arce 2013Document14 pagesFibrillation Auriculaire Arce 2013nemeyechrisbelPas encore d'évaluation
- Laudition Au Cours de La Polyarthrite RhumatoideDocument9 pagesLaudition Au Cours de La Polyarthrite RhumatoideKate ClarksonPas encore d'évaluation
- Article07 24Document6 pagesArticle07 24ACEEE AssistPas encore d'évaluation
- Le Profil Epidemiologique Et La Prise en Charge Des Perforations Greliques Post-Traumatiques A Propos de 50 CasDocument5 pagesLe Profil Epidemiologique Et La Prise en Charge Des Perforations Greliques Post-Traumatiques A Propos de 50 CasIJAR JOURNALPas encore d'évaluation
- Apport de La Tomodensitomètrie Dans Le Diagnostic Des AccidentDocument5 pagesApport de La Tomodensitomètrie Dans Le Diagnostic Des AccidentMüs Tã PhåPas encore d'évaluation
- Bilan Étiologique Des AVC Ischémiques: Le DossierDocument3 pagesBilan Étiologique Des AVC Ischémiques: Le Dossierbenelmouffok samiaPas encore d'évaluation
- Dysplasie Arythmogene de Ventricule Droit Revelee Par Une Tachycardie Ventriculaire Chez Un Sujet JeuneDocument6 pagesDysplasie Arythmogene de Ventricule Droit Revelee Par Une Tachycardie Ventriculaire Chez Un Sujet JeuneIJAR JOURNALPas encore d'évaluation
- VIGNETTE CLINIQUE-afraDocument5 pagesVIGNETTE CLINIQUE-afraAmenElleh ShilPas encore d'évaluation
- Traitement Selon Cours PR MahiDocument40 pagesTraitement Selon Cours PR MahiABDELLAH REZZIKIPas encore d'évaluation
- L’émergence de la médecine scientifique: Sciences et philosophieD'EverandL’émergence de la médecine scientifique: Sciences et philosophiePas encore d'évaluation
- Revue Générale Des Troubles Anxieux - Troubles Psychiatriques - Édition Professionnelle Du Manuel MSDDocument4 pagesRevue Générale Des Troubles Anxieux - Troubles Psychiatriques - Édition Professionnelle Du Manuel MSDMalak GabsiPas encore d'évaluation
- 6.1.1.allergie Alimentaire Chez L Adulte Et L EnfantDocument9 pages6.1.1.allergie Alimentaire Chez L Adulte Et L EnfantSsMm MessyPas encore d'évaluation
- Abg STD FinalDocument83 pagesAbg STD Finalyoussef karamPas encore d'évaluation
- Immunotherapie Doc FinalDocument3 pagesImmunotherapie Doc FinalFaisal MajzoubPas encore d'évaluation
- Syndrome de West - Rapport de StageDocument70 pagesSyndrome de West - Rapport de StageDamya SlimaniPas encore d'évaluation
- DCPE 572 Annexe V.2.12.2021Document1 pageDCPE 572 Annexe V.2.12.2021BadreddinePas encore d'évaluation
- 06-Introduction À La PsychiatrieDocument6 pages06-Introduction À La PsychiatrieNoureddine BoulaouedPas encore d'évaluation
- Impact Internat - Neurologie PDFDocument118 pagesImpact Internat - Neurologie PDFkhealouPas encore d'évaluation
- Les TiquesDocument16 pagesLes TiquesAlmenaouar AdelPas encore d'évaluation
- Introduction Semiologie PediatriqueDocument34 pagesIntroduction Semiologie PediatriqueIdrissou Fmsb80% (5)
- Institut Privé Profession de La SantéDocument7 pagesInstitut Privé Profession de La SantéChaimae SghairPas encore d'évaluation
- L'héminégligence: Prise en Charge KinésithérapiqueDocument42 pagesL'héminégligence: Prise en Charge KinésithérapiqueAymen DabboussiPas encore d'évaluation
- Memoire Arouss AychaDocument27 pagesMemoire Arouss AychaAycha AroussePas encore d'évaluation
- Richaud 2010Document5 pagesRichaud 2010Hèla HassenPas encore d'évaluation
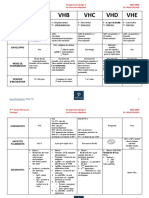
- TD2 HV (A, B, C, D, E)Document3 pagesTD2 HV (A, B, C, D, E)Hichem KenounPas encore d'évaluation
- Drainage 4Document25 pagesDrainage 4Khalil IbrahimPas encore d'évaluation
- Dzexams 2as Francais As - d1 20190 519874Document2 pagesDzexams 2as Francais As - d1 20190 519874Belabes TarayadPas encore d'évaluation
- OstéonécroseDocument62 pagesOstéonécroseMathieu DauradePas encore d'évaluation
- 131 Poly 1 PDFDocument34 pages131 Poly 1 PDFAdel KchoukPas encore d'évaluation
- Guide Urgences Pédiatriques 2017Document267 pagesGuide Urgences Pédiatriques 2017Sadio Ousmane DiédhiouPas encore d'évaluation
- Exercice Word 2 Journée de Formation Fini PDFDocument2 pagesExercice Word 2 Journée de Formation Fini PDFMohamed Aly SowPas encore d'évaluation
- 6 - Angicholites AiguesDocument2 pages6 - Angicholites AiguesKarimBenAPas encore d'évaluation
- Les Syndromes GlomérulairesDocument9 pagesLes Syndromes GlomérulairesNour-El ImanePas encore d'évaluation
- HMG Douloureuse EMCDocument20 pagesHMG Douloureuse EMCsanaa berPas encore d'évaluation
- Cas Clinique Acidocetose DiabetiqueDocument57 pagesCas Clinique Acidocetose Diabetiquesam nehPas encore d'évaluation
- Projet 7500Document10 pagesProjet 7500Marc KonanPas encore d'évaluation
- Gynécologie Pédiatrie Et GénétiqueDocument127 pagesGynécologie Pédiatrie Et Génétiquearmel TOMMEPas encore d'évaluation
- Aide Memire D'hematologieDocument266 pagesAide Memire D'hematologiesa kaPas encore d'évaluation
- Rapport SFO 2017 - OPHTALMOLOGIE PÉDIATRIQUE PDFDocument103 pagesRapport SFO 2017 - OPHTALMOLOGIE PÉDIATRIQUE PDFTieni DembéléPas encore d'évaluation
- Hématologie Adulte Et Pédiatrique, Onco-Hématologie R2C 2021Document413 pagesHématologie Adulte Et Pédiatrique, Onco-Hématologie R2C 2021Iheb KarâaPas encore d'évaluation