Vous aimerez peut-être aussi
- Memoire Fin D'étudeDocument38 pagesMemoire Fin D'étudeJoao Tio MendesPas encore d'évaluation
- Urgences Spécifiques en Oncologie ThoraciqueDocument28 pagesUrgences Spécifiques en Oncologie ThoraciqueLoulou popPas encore d'évaluation
- Cours Infirmier TransplantationDocument20 pagesCours Infirmier Transplantationhela bergaouiPas encore d'évaluation
- Cours Infirmier TransplantationDocument20 pagesCours Infirmier TransplantationibtihelantriPas encore d'évaluation
- NeurologieDocument11 pagesNeurologieمحمد شوقيPas encore d'évaluation
- PALUDISMEDocument22 pagesPALUDISMEAbenekPas encore d'évaluation
- PaludismeDocument40 pagesPaludismeMrTriumphant100% (3)
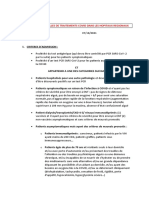
- 71021protocole de Traitements Covid Dans Les Hopitaux RegionauxDocument7 pages71021protocole de Traitements Covid Dans Les Hopitaux RegionauxStonefalconPas encore d'évaluation
- 05 Drépanocytose Et Grossesse - Protocole GGOLFB 2017Document5 pages05 Drépanocytose Et Grossesse - Protocole GGOLFB 2017Stéphane DonohPas encore d'évaluation
- Cat NeurologieDocument11 pagesCat NeurologieH GooPas encore d'évaluation
- CAT Devant Une TBCDocument3 pagesCAT Devant Une TBCGrace KellyPas encore d'évaluation
- 2015 11 Protocole Parcours de Soins VFDocument12 pages2015 11 Protocole Parcours de Soins VFzouiche KhadidjaPas encore d'évaluation
- Corrigé Des TRAVAUX DIRIGÉS 3 Et 4 Année 2022Document7 pagesCorrigé Des TRAVAUX DIRIGÉS 3 Et 4 Année 2022SOphieSat100% (1)
- Cat Neonat ModifiéDocument75 pagesCat Neonat ModifiéAbdelghani InousPas encore d'évaluation
- OapDocument5 pagesOapLuc TiendrebeogoPas encore d'évaluation
- Traitement Des Exacerbations Aigues Des BPCODocument6 pagesTraitement Des Exacerbations Aigues Des BPCOedhazard1988Pas encore d'évaluation
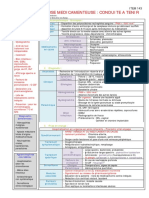
- Les Conduites À Tenir en InfectieuxDocument43 pagesLes Conduites À Tenir en Infectieuxقريوي مصطفىPas encore d'évaluation
- Protocole Therapeutique Pour La Prise en Charge Ambulatoire Du Covid-19 A L'Ihu Mediterranee Infection 29 JANVIER 2021Document6 pagesProtocole Therapeutique Pour La Prise en Charge Ambulatoire Du Covid-19 A L'Ihu Mediterranee Infection 29 JANVIER 2021no pain no gainPas encore d'évaluation
- Urgences CAT Très PratiqueDocument49 pagesUrgences CAT Très PratiqueAbdelkader Hocini50% (2)
- PEC Gestante Covid 10092021Document11 pagesPEC Gestante Covid 10092021CristinaCaprosPas encore d'évaluation
- Asthme Aigu Grave 2017 PDFDocument46 pagesAsthme Aigu Grave 2017 PDFSerigne Sohibou GayePas encore d'évaluation
- Le Guide Des Anti-InfectieuxDocument97 pagesLe Guide Des Anti-InfectieuxChrist en ellePas encore d'évaluation
- TD12 TransfusionDocument22 pagesTD12 TransfusionAbderrahmenPas encore d'évaluation
- Eclampsie en ReanimationDocument29 pagesEclampsie en ReanimationEbePas encore d'évaluation
- UntitledDocument282 pagesUntitledThe Curious الفضوليPas encore d'évaluation
- Drepanocytose Cas Clinique PediatrieDocument16 pagesDrepanocytose Cas Clinique PediatrieEya EL KAMELPas encore d'évaluation
- Syndrome ThoraciqueDocument3 pagesSyndrome ThoraciqueganlibalamPas encore d'évaluation
- KHH Handbook 2020Document69 pagesKHH Handbook 2020saraliciatinahPas encore d'évaluation
- Primaquine PEC en Zone D'éliminationDocument42 pagesPrimaquine PEC en Zone D'éliminationDdsn DibaPas encore d'évaluation
- Compile Des CAT - CopieDocument21 pagesCompile Des CAT - CopieYoussra haderPas encore d'évaluation
- Malaria TTT Urgences Rev-2021Document7 pagesMalaria TTT Urgences Rev-2021stephanekoffi16Pas encore d'évaluation
- BonUsageAntibiotiques1 PDFDocument40 pagesBonUsageAntibiotiques1 PDFMamadou MbaoPas encore d'évaluation
- Spilf Groupe Reco Spilf Icd Escmid 2022Document10 pagesSpilf Groupe Reco Spilf Icd Escmid 2022jean duval destinPas encore d'évaluation
- Protocole de Prise en Charge Des Pathologies en Pediatrie IDocument11 pagesProtocole de Prise en Charge Des Pathologies en Pediatrie IAbba aliPas encore d'évaluation
- Choc Et Pancreatite AigueDocument39 pagesChoc Et Pancreatite AiguePauline SeignéPas encore d'évaluation
- PaludismeDocument33 pagesPaludismeLeonel TamaPas encore d'évaluation
- Protocole Therapeutique Chirurgie AntsirabeDocument21 pagesProtocole Therapeutique Chirurgie AntsirabenaydandomalalaPas encore d'évaluation
- Item 143 Agranulocytose Medicamenteuse PDFDocument1 pageItem 143 Agranulocytose Medicamenteuse PDFPetit Suisse FramboiséPas encore d'évaluation
- Referents2009 Atelier Atb GeriatrieDocument64 pagesReferents2009 Atelier Atb GeriatrieMeriem HoudaPas encore d'évaluation
- PaludismeDocument3 pagesPaludismeAlaa SobhiPas encore d'évaluation
- Livret Internes 20111128135420Document226 pagesLivret Internes 20111128135420gabi38100% (1)
- Jni2017 Ei StradyDocument33 pagesJni2017 Ei StradyRima RimaPas encore d'évaluation
- DIU Réa Médicaments en Cardiologie PédiatriqueDocument91 pagesDIU Réa Médicaments en Cardiologie PédiatriqueYoucef KelkouliPas encore d'évaluation
- PheoDocument42 pagesPheoSi LaPas encore d'évaluation
- CAS CLINIQAUEJUIN 2014 Nouveau Document Microsoft Office Word - PDF FilenameDocument10 pagesCAS CLINIQAUEJUIN 2014 Nouveau Document Microsoft Office Word - PDF FilenameAnis Ali-khodjaPas encore d'évaluation
- Cat Devant UnemeningiteDocument34 pagesCat Devant UnemeningiteSaid AssowehPas encore d'évaluation
- Exercices Evcf Et Evcp TinaDocument246 pagesExercices Evcf Et Evcp TinaLarbi Bouamrane AbdelkaderPas encore d'évaluation
- N°6 Intox Au ParacetamolDocument29 pagesN°6 Intox Au ParacetamolYacouba DembelePas encore d'évaluation
- Cas Cliniques ToxicoDocument75 pagesCas Cliniques ToxicoAya Eljazouli100% (1)
- Cardiomyopathie Du PrripztDocument15 pagesCardiomyopathie Du PrripztTHERESE BEHEPas encore d'évaluation
- PreeclampsieDocument46 pagesPreeclampsieManel KammounPas encore d'évaluation
- PaludismeDocument33 pagesPaludismeYounesPas encore d'évaluation
- CAS CLINIQAUE Nouveau Document Microsoft Office Word - PDF Filename UTF-8''CDocument9 pagesCAS CLINIQAUE Nouveau Document Microsoft Office Word - PDF Filename UTF-8''CAnis Ali-khodjaPas encore d'évaluation
- Protocole CHU PE - HTA GravidiqueDocument6 pagesProtocole CHU PE - HTA Gravidiquenganvtk.hmuPas encore d'évaluation
- Les Médicaments de L'hémostaseDocument10 pagesLes Médicaments de L'hémostaseLahcen ElmoumouPas encore d'évaluation
- Compte Rendu D'hospitalisationDocument6 pagesCompte Rendu D'hospitalisationAmir Na DzPas encore d'évaluation
- Emergency GuidelinesDocument11 pagesEmergency GuidelinesamirwassiPas encore d'évaluation
- Examen LaboDocument66 pagesExamen LaboGhizlan GharibPas encore d'évaluation
- Doc4 Suivi Therapeutique Pharmacologique ISDocument20 pagesDoc4 Suivi Therapeutique Pharmacologique ISMou SinayPas encore d'évaluation
- Les thérapies ciblées modernes du cancer du sein : mécanismes et application cliniqueD'EverandLes thérapies ciblées modernes du cancer du sein : mécanismes et application cliniquePas encore d'évaluation
- 7.hydrocéphalie de L'enfant Et NourissonDocument46 pages7.hydrocéphalie de L'enfant Et NourissonAlpha BaPas encore d'évaluation
- 13-10-14 Syndrome Inflammatoire Mise Au PointDocument121 pages13-10-14 Syndrome Inflammatoire Mise Au Pointjacques yiborPas encore d'évaluation
- Fibromyalgie 5Document7 pagesFibromyalgie 5sylvain bergPas encore d'évaluation
- 2005 06 14 Urgences Chez Patient Cirrhotique DR J-P MULKAYDocument5 pages2005 06 14 Urgences Chez Patient Cirrhotique DR J-P MULKAYNoadia RafararisonPas encore d'évaluation
- Affiche Infection MFA BRDocument1 pageAffiche Infection MFA BRdelfinnePas encore d'évaluation
- PéritonitesDocument16 pagesPéritonitesMohamed BoudouPas encore d'évaluation
- EBOOK Pascal Boniface - Geopolitique Du Covid-19 PDFDocument55 pagesEBOOK Pascal Boniface - Geopolitique Du Covid-19 PDFstaros100% (2)
- m2 Semio Sémiologie de La FièvreDocument34 pagesm2 Semio Sémiologie de La Fièvreأغا ني100% (1)
- Les Tendinites Des Fléchisseurs Au Poignet Et À La MainDocument16 pagesLes Tendinites Des Fléchisseurs Au Poignet Et À La MainurgencemainnicePas encore d'évaluation
- Planche Dépression CaractériséeDocument5 pagesPlanche Dépression CaractériséeSamia BelabbasPas encore d'évaluation
- Le Diabète 2020Document9 pagesLe Diabète 2020Hanane JibetPas encore d'évaluation
- Révision 3 Internes Avec CorrigéDocument10 pagesRévision 3 Internes Avec CorrigéRamzi RzPas encore d'évaluation
- Esprit Metaphore SanteDocument8 pagesEsprit Metaphore SantegrubanPas encore d'évaluation
- Tableau Folie Naheulbeuk JDR PDFDocument1 pageTableau Folie Naheulbeuk JDR PDFSolène BouillonPas encore d'évaluation
- Cour 01 Toxico DefinitionDocument9 pagesCour 01 Toxico DefinitionBrandon AustinPas encore d'évaluation
- 00 917Document9 pages00 917hizballah27Pas encore d'évaluation
- Introduction À La Semiologie NeurologiqueDocument12 pagesIntroduction À La Semiologie NeurologiqueSekou BoiguilePas encore d'évaluation
- Guide de PEC Des Méningite PurulenteDocument69 pagesGuide de PEC Des Méningite Purulentechouli mohamedPas encore d'évaluation
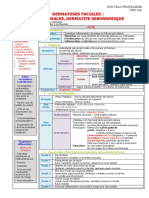
- 109 Dermatoses Faciales Acne - , Rosace - E, Dermatite Se - Borrhe - IqueDocument3 pages109 Dermatoses Faciales Acne - , Rosace - E, Dermatite Se - Borrhe - IqueAboubacar SomparePas encore d'évaluation
- Insuffisance Cardiaque de LDocument10 pagesInsuffisance Cardiaque de LAsma BdfPas encore d'évaluation
- 20-Infection À VIH - 2017Document12 pages20-Infection À VIH - 2017Sebbar SebbardPas encore d'évaluation
- Wcms 301237Document97 pagesWcms 301237chelcy kezetminPas encore d'évaluation
- Sf1 Resume FeedbackDocument15 pagesSf1 Resume FeedbackKhadija Barro ComptepleinPas encore d'évaluation
- Rsca 1Document9 pagesRsca 1Mohammed BoumlikPas encore d'évaluation
- Péricardites Mai 2023 Final-1Document20 pagesPéricardites Mai 2023 Final-1Lamine SavadogoPas encore d'évaluation
- Cancer Du ReinDocument27 pagesCancer Du ReinBelhadj AyoubPas encore d'évaluation
- Richaud 2010Document5 pagesRichaud 2010Hèla HassenPas encore d'évaluation
- 4 - ParamyxovirusDocument47 pages4 - ParamyxovirusIman Ahmed100% (3)
- Bible Medecine Interne Finale (Gratien) - 115141Document270 pagesBible Medecine Interne Finale (Gratien) - 115141Joel IrakizaPas encore d'évaluation
- Emm 117Document116 pagesEmm 117Boubacar IbrahimPas encore d'évaluation