Vous aimerez peut-être aussi
- Conduite À Tenir Devant Une Tumeur Kystique Du PancréasDocument5 pagesConduite À Tenir Devant Une Tumeur Kystique Du PancréashoangducnamPas encore d'évaluation
- Apport de l'IRM Dans Les Cancers Utérins: TechniqueDocument10 pagesApport de l'IRM Dans Les Cancers Utérins: TechniquekydPas encore d'évaluation
- LE DEPISTAGE DES CANCERS L'exemple Du Cancer Du Sein EXPERIENCE DE L'ASSOCIATION DAR ELAMAL DE LUTTE CONTRE LE CANCERDocument51 pagesLE DEPISTAGE DES CANCERS L'exemple Du Cancer Du Sein EXPERIENCE DE L'ASSOCIATION DAR ELAMAL DE LUTTE CONTRE LE CANCERDr Riyadh ESSEFIPas encore d'évaluation
- IRM Cancer EndomètreDocument5 pagesIRM Cancer EndomètreFabrice DjekPas encore d'évaluation
- Cat Devant Un Nodule Mamma I ReDocument36 pagesCat Devant Un Nodule Mamma I ReHind EssalimPas encore d'évaluation
- Ref Sein 2011Document32 pagesRef Sein 2011menar moussaouiPas encore d'évaluation
- 14 PR David GROHEUX Imagerie Par Medecine Nucleaire Et Seins IMAGERIE PAR MEDECINE NUCLEAIRE ET CANCER DU SEINDocument127 pages14 PR David GROHEUX Imagerie Par Medecine Nucleaire Et Seins IMAGERIE PAR MEDECINE NUCLEAIRE ET CANCER DU SEINelsilicarvalho12Pas encore d'évaluation
- 56 Irm Fonctionnelle de Prostate 07Document18 pages56 Irm Fonctionnelle de Prostate 07CIM JasminsPas encore d'évaluation
- 1-S2.0-S2049080122014534-Main FRDocument9 pages1-S2.0-S2049080122014534-Main FREleonore Marcelle Akissi Agni Ola SourouppPPas encore d'évaluation
- 2015 RPC Sein Tumeurs BenignesDocument33 pages2015 RPC Sein Tumeurs BenignesNacima Nait AbdelazizPas encore d'évaluation
- Carcinomepapillairesereuxlocalementavance Du Coluterin: A Propos Dun Casclinique Rare Et Revue de La LitteratureDocument5 pagesCarcinomepapillairesereuxlocalementavance Du Coluterin: A Propos Dun Casclinique Rare Et Revue de La LitteratureIJAR JOURNALPas encore d'évaluation
- PLACSIS09Document16 pagesPLACSIS09houssein.hajj.mdPas encore d'évaluation
- Les Tumeurs Intracanalaires Papillaires Et Mucineuses Du Pancreas Multifocales: Prise en Charge Et Alternatives Therapeutiques PossiblesDocument9 pagesLes Tumeurs Intracanalaires Papillaires Et Mucineuses Du Pancreas Multifocales: Prise en Charge Et Alternatives Therapeutiques PossiblesIJAR JOURNALPas encore d'évaluation
- Sein Principes de Prise en Charge Version 373 Publiee Du 10 01 2020 PDFDocument112 pagesSein Principes de Prise en Charge Version 373 Publiee Du 10 01 2020 PDFkassem989Pas encore d'évaluation
- MammographieDocument8 pagesMammographieasdfPas encore d'évaluation
- Cancer Du SeinDocument14 pagesCancer Du SeinSerigne Sohibou GayePas encore d'évaluation
- Le Microcarcinome MammaireDocument27 pagesLe Microcarcinome MammaireSalim LoudjediPas encore d'évaluation
- Tele MammograpieDocument1 pageTele MammograpieOmar ChamakhPas encore d'évaluation
- Sein Principes de Prise en Charge Version 416 Publiee Du 28 02 2022Document118 pagesSein Principes de Prise en Charge Version 416 Publiee Du 28 02 2022Moatez HlmPas encore d'évaluation
- Balleyguier2013 2Document10 pagesBalleyguier2013 2abdoulePas encore d'évaluation
- Diagnostic Des Cancers2Document30 pagesDiagnostic Des Cancers2Ali CiaPas encore d'évaluation
- Pénectomie Partielle Pour Un Carcinome de La Verge: A Propos de 24 CasDocument4 pagesPénectomie Partielle Pour Un Carcinome de La Verge: A Propos de 24 CasIOSRjournalPas encore d'évaluation
- 3S2 - Cours Imagérie MédicaleDocument58 pages3S2 - Cours Imagérie MédicaleMoTaALPas encore d'évaluation
- Cancer Du Sein FINALDocument49 pagesCancer Du Sein FINALanis anisPas encore d'évaluation
- Decrevoisier2016 PDFDocument9 pagesDecrevoisier2016 PDFface bookPas encore d'évaluation
- Place de L - Imagerie de Perfusion Par Irm Dans La Prise en Charge Des Tumeurs CérébralesDocument12 pagesPlace de L - Imagerie de Perfusion Par Irm Dans La Prise en Charge Des Tumeurs Cérébralesgeorgiana MariaPas encore d'évaluation
- Apport de L'échographie Doppler Pour La GynécologieDocument12 pagesApport de L'échographie Doppler Pour La GynécologieYounes AGIPas encore d'évaluation
- Hesav TB Beguin 2014Document62 pagesHesav TB Beguin 2014abdoPas encore d'évaluation
- GU Microanévrysme Associés Aux Angiomyolipomes RénauxDocument35 pagesGU Microanévrysme Associés Aux Angiomyolipomes Rénauxمحمد كبيدةPas encore d'évaluation
- ColpoDocument3 pagesColposaffkhal ottPas encore d'évaluation
- 40-Texte de L'article-99-1-10-20200521Document4 pages40-Texte de L'article-99-1-10-20200521saad ziadiPas encore d'évaluation
- Cancer Du Col UtérinDocument8 pagesCancer Du Col UtérinDoc AsmaPas encore d'évaluation
- Cancerologie Polycopie Tumeurs Col Et Corps UterinDocument19 pagesCancerologie Polycopie Tumeurs Col Et Corps UterinRoxanaHliboceanuPas encore d'évaluation
- Traitement Conservateur Des Cancers Du SeinDocument6 pagesTraitement Conservateur Des Cancers Du SeinpingusPas encore d'évaluation
- PDF - Vol 98-11-N°11Document9 pagesPDF - Vol 98-11-N°11kepipranave-9084Pas encore d'évaluation
- Articles Originaux: Mali Médical 2006 T Xxi #3 43Document7 pagesArticles Originaux: Mali Médical 2006 T Xxi #3 43agbokannou spéroPas encore d'évaluation
- Cancer de L'oesophageDocument39 pagesCancer de L'oesophageaitsurgery4730100% (2)
- Imagerie Et Cardiologie Interventionnelle: SciencedirectDocument2 pagesImagerie Et Cardiologie Interventionnelle: SciencedirectMoncef PechaPas encore d'évaluation
- GU IRM Prostatique MultiparamétriqueDocument61 pagesGU IRM Prostatique Multiparamétriqueمحمد كبيدةPas encore d'évaluation
- Profil Scanographique Des Tumeurs Du PancreasDocument8 pagesProfil Scanographique Des Tumeurs Du PancreasKarim TorressPas encore d'évaluation
- MXT05 Hamrioui Et MayoufDocument2 pagesMXT05 Hamrioui Et MayoufDoctoresse FugitivePas encore d'évaluation
- RADIOLOGIE ET IMAGERIE MÉDICALE Génito-Urinaire - Gynéco-Obstétricale - Mammaire Mise À Jour IV-2021Document36 pagesRADIOLOGIE ET IMAGERIE MÉDICALE Génito-Urinaire - Gynéco-Obstétricale - Mammaire Mise À Jour IV-2021yachamidPas encore d'évaluation
- Carcinome Papillaire Intra-Kystique Du Sein: Quelle Indication de La Radiotherapie? A Travers Un Cas Clinique Et Une Revue de La LitteratureDocument4 pagesCarcinome Papillaire Intra-Kystique Du Sein: Quelle Indication de La Radiotherapie? A Travers Un Cas Clinique Et Une Revue de La LitteratureIJAR JOURNALPas encore d'évaluation
- Échographie Endovaginale Doppler 3d 2022Document335 pagesÉchographie Endovaginale Doppler 3d 2022KalabaPas encore d'évaluation
- La Prise en Charge Des Tumeurs Neuro Endocrines Du Col Uterin: A Propos Dun Cas Et Une Revue de La LitteratureDocument5 pagesLa Prise en Charge Des Tumeurs Neuro Endocrines Du Col Uterin: A Propos Dun Cas Et Une Revue de La LitteratureIJAR JOURNALPas encore d'évaluation
- Carcinome Mucineux Du Sein: A Propos de 13 Cas Et Revue de La LitteratureDocument5 pagesCarcinome Mucineux Du Sein: A Propos de 13 Cas Et Revue de La LitteratureIJAR JOURNALPas encore d'évaluation
- NL 11 IA Et Imagerie Medicale RS ED LF 1 PDFDocument9 pagesNL 11 IA Et Imagerie Medicale RS ED LF 1 PDFkarima hadirPas encore d'évaluation
- Capture D'écran . 2022-11-30 À 12.46.06Document1 pageCapture D'écran . 2022-11-30 À 12.46.06BOUDHARPas encore d'évaluation
- Medecine Nucleaire-2Document9 pagesMedecine Nucleaire-2Donatien MukazPas encore d'évaluation
- Les Cancers Gynécologiques: Cours D'oncologie Médicale Undh-Fmss Dcem4 DR Joseph BERNARD JRDocument48 pagesLes Cancers Gynécologiques: Cours D'oncologie Médicale Undh-Fmss Dcem4 DR Joseph BERNARD JRGroupe 6 Internat UNDHPas encore d'évaluation
- GYO-Cancer Du Sein (Anapath)Document47 pagesGYO-Cancer Du Sein (Anapath)Wilfried AboPas encore d'évaluation
- Article. Réévaluation en IRM Apres Traitement Neoadjuvant Du Cancer Rectal 2016Document9 pagesArticle. Réévaluation en IRM Apres Traitement Neoadjuvant Du Cancer Rectal 2016Trí Cương NguyễnPas encore d'évaluation
- IntroductionDocument25 pagesIntroductionnouryasmine0220Pas encore d'évaluation
- RDP 2018 1 41Document15 pagesRDP 2018 1 41Amine DounanePas encore d'évaluation
- Vidal Recos - 08 Hépato Gastro EntérologieDocument111 pagesVidal Recos - 08 Hépato Gastro EntérologieCherraben Taha AminePas encore d'évaluation
- ImagerieDocument8 pagesImagerieakremcoolPas encore d'évaluation
- Maladie Micrométastatique Et Maladie Résiduelle Axillaire. Exemple Du Cancer Du SeinDocument5 pagesMaladie Micrométastatique Et Maladie Résiduelle Axillaire. Exemple Du Cancer Du SeinJean-Philippe BinderPas encore d'évaluation
- Radiographie GeneraleDocument11 pagesRadiographie GeneraleNoureddine BenarifaPas encore d'évaluation
- Dossier Documentaire ImagerieDocument15 pagesDossier Documentaire ImagerieEric Valery TAHOUE NOUMSIPas encore d'évaluation
- Grand Support Chirurgie VisceraleDocument219 pagesGrand Support Chirurgie VisceraleNizar KaddiouiPas encore d'évaluation
- Réponse AntitumoraleDocument58 pagesRéponse AntitumoraleMaï Ssa100% (1)
- Terminologie CancérologieDocument2 pagesTerminologie CancérologieVELCOFPas encore d'évaluation
- Cours Ana-Path Tumeurs Glandulaires 1Document64 pagesCours Ana-Path Tumeurs Glandulaires 1Aicha MadiPas encore d'évaluation
- Cancerologie - MEDLINEDocument425 pagesCancerologie - MEDLINELilya Med NinaPas encore d'évaluation
- Cellule CancéreuseDocument49 pagesCellule CancéreuseSerigne Sohibou GayePas encore d'évaluation
- Mémoir Sur Les MTDocument51 pagesMémoir Sur Les MTzaraPas encore d'évaluation
- 12 Cancer Du Cavum2020Document21 pages12 Cancer Du Cavum2020Mouhamed Amine SeddikPas encore d'évaluation
- French 1lit18 1trim d2Document2 pagesFrench 1lit18 1trim d2hisokaPas encore d'évaluation
- 05 AFeydy - Sémiologie TDM IRM Squelette Axial - Optionnel DES MN - 16&170518 PDFDocument119 pages05 AFeydy - Sémiologie TDM IRM Squelette Axial - Optionnel DES MN - 16&170518 PDFNarcisse NwedjiwePas encore d'évaluation
- Cancer Du Col UtérinDocument29 pagesCancer Du Col Utérinanis anisPas encore d'évaluation
- Les Tumeurs OvariennesDocument7 pagesLes Tumeurs OvariennesMohamed IkbalPas encore d'évaluation
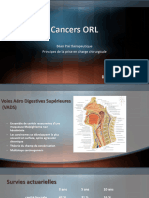
- Cancers ORL: Bilan Pré Thérapeutique Principes de La Prise en Charge ChirurgicaleDocument42 pagesCancers ORL: Bilan Pré Thérapeutique Principes de La Prise en Charge ChirurgicaleSpisie MikePas encore d'évaluation
- Cancer Du Poumon - Support de CoursDocument92 pagesCancer Du Poumon - Support de CoursMarouan DhnPas encore d'évaluation
- La Qualité de Vie Chez Les Femmes Atteintes Du Cancer Du Sein OpéréesDocument131 pagesLa Qualité de Vie Chez Les Femmes Atteintes Du Cancer Du Sein OpéréesHamza MoustakimPas encore d'évaluation
- 01 - Eviter Le CancerDocument11 pages01 - Eviter Le CancerStefaniaPas encore d'évaluation
- Cancer Du PoumonDocument25 pagesCancer Du PoumonBelhadj AyoubPas encore d'évaluation
- Masses Abdominale de LenfantDocument44 pagesMasses Abdominale de LenfantElyes ZoghlamiPas encore d'évaluation
- Ampullectomie ChirurgicaleDocument7 pagesAmpullectomie ChirurgicaleREBBANI MohammedPas encore d'évaluation
- 2001 A 2 Lipome LiposarcomeDocument12 pages2001 A 2 Lipome LiposarcomeVladlena CaraimanPas encore d'évaluation
- Cancer Du Sein 2018Document37 pagesCancer Du Sein 2018haj khlifa saraPas encore d'évaluation
- Cancer Bronchique 20 03 14 FACDocument43 pagesCancer Bronchique 20 03 14 FACFethi SerayaPas encore d'évaluation
- Referentiel Senorif 2021 2022Document188 pagesReferentiel Senorif 2021 2022douaePas encore d'évaluation
- Cancer de L'oesophageDocument34 pagesCancer de L'oesophageDean WinchesterPas encore d'évaluation
- ADP Et TM Du CouDocument13 pagesADP Et TM Du CouSalim MedjmadjPas encore d'évaluation
- Tumefactions CervicaleDocument10 pagesTumefactions CervicaleHalla BennaaPas encore d'évaluation
- Cancer Du PancréasDocument4 pagesCancer Du PancréasREGIS KAMBIREPas encore d'évaluation
- Place de L - Imagerie de Perfusion Par Irm Dans La Prise en Charge Des Tumeurs CérébralesDocument12 pagesPlace de L - Imagerie de Perfusion Par Irm Dans La Prise en Charge Des Tumeurs Cérébralesgeorgiana MariaPas encore d'évaluation
- Cancer Du Sinus PiriformeDocument4 pagesCancer Du Sinus Piriformeadelmiringui2Pas encore d'évaluation
- Lymphome DE HODGKINDocument22 pagesLymphome DE HODGKINSalomon JosephPas encore d'évaluation
- 20 Véritables remèdes de nos grands-mères pour maigrir vite et enfin perdre du poidsD'Everand20 Véritables remèdes de nos grands-mères pour maigrir vite et enfin perdre du poidsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Beauté Santé: 107 Recettes faciles de produits cosmétiques bio à faire vous-mêmes avec les ingrédients de votre cuisine !D'EverandBeauté Santé: 107 Recettes faciles de produits cosmétiques bio à faire vous-mêmes avec les ingrédients de votre cuisine !Évaluation : 5 sur 5 étoiles5/5 (1)
- LE PLACEBO, C'EST VOUS !: Comment donner le pouvoir à votre espritD'EverandLE PLACEBO, C'EST VOUS !: Comment donner le pouvoir à votre espritPas encore d'évaluation
- Régime Charge Glycémique, Régime Express IG: Perdre 10 kg et vivre 10 ans de plus ! + 39 Recettes IG basD'EverandRégime Charge Glycémique, Régime Express IG: Perdre 10 kg et vivre 10 ans de plus ! + 39 Recettes IG basÉvaluation : 5 sur 5 étoiles5/5 (3)
- Manuel pour les débutants Fabriquez des savons naturelsD'EverandManuel pour les débutants Fabriquez des savons naturelsÉvaluation : 3 sur 5 étoiles3/5 (2)
- Géobiologie de l'habitat et Géobiologie sacrée: Pour un lieu sainD'EverandGéobiologie de l'habitat et Géobiologie sacrée: Pour un lieu sainÉvaluation : 4.5 sur 5 étoiles4.5/5 (2)
- Encyclopédie de la thérapie par ventouses : Une nouvelle éditionD'EverandEncyclopédie de la thérapie par ventouses : Une nouvelle éditionPas encore d'évaluation
- Régime Cétogène: Le Guide Ultime Pour Maîtriser Une Perte De Poids Saine (Recettes De Régime Céto)D'EverandRégime Cétogène: Le Guide Ultime Pour Maîtriser Une Perte De Poids Saine (Recettes De Régime Céto)Pas encore d'évaluation
- La maîtrise de soi-même par l'autosuggestion consciente: la méthode CouéD'EverandLa maîtrise de soi-même par l'autosuggestion consciente: la méthode CouéPas encore d'évaluation
- Pour Maigrir: 67 recettes faciles de Jus de Fruits et de Légumes Crus Détox pour perdre du poidsD'EverandPour Maigrir: 67 recettes faciles de Jus de Fruits et de Légumes Crus Détox pour perdre du poidsÉvaluation : 5 sur 5 étoiles5/5 (2)
- Ces aliments qui font maigrir: Surveiller son alimentation pour perdre du poidsD'EverandCes aliments qui font maigrir: Surveiller son alimentation pour perdre du poidsPas encore d'évaluation
- Nourrir mon Enfant intérieur: L'anti-régime d'une diététicienne épicurienneD'EverandNourrir mon Enfant intérieur: L'anti-régime d'une diététicienne épicurienneÉvaluation : 5 sur 5 étoiles5/5 (1)
- 100 Santé Smoothie Recettes Pour Détoxifier Et Pour Plus De Vitalité: (Guide Diététique Pour Perdre Du Poids Etse Sentir Bien Dans Son Corps)D'Everand100 Santé Smoothie Recettes Pour Détoxifier Et Pour Plus De Vitalité: (Guide Diététique Pour Perdre Du Poids Etse Sentir Bien Dans Son Corps)Pas encore d'évaluation
- Pendule et magnétisme: 2 guides en 1D'EverandPendule et magnétisme: 2 guides en 1Évaluation : 5 sur 5 étoiles5/5 (1)
- Jeûne Intermittent, Fasting : L’ultime guide de la méthode la plus efficace pour perdre du poids naturellement, gagner en énergie et vivre plus longtemps en meilleure santéD'EverandJeûne Intermittent, Fasting : L’ultime guide de la méthode la plus efficace pour perdre du poids naturellement, gagner en énergie et vivre plus longtemps en meilleure santéÉvaluation : 2.5 sur 5 étoiles2.5/5 (2)
- Chirologie radiesthésique: Analyse de la main et de son auraD'EverandChirologie radiesthésique: Analyse de la main et de son auraPas encore d'évaluation
- La réflexologie et ses bienfaits: Une médecine alternative pour avoir une bonne hygiène de vieD'EverandLa réflexologie et ses bienfaits: Une médecine alternative pour avoir une bonne hygiène de viePas encore d'évaluation
- Comment perdre la graisse du ventre En français/ How To Lose Belly Fat In FrenchD'EverandComment perdre la graisse du ventre En français/ How To Lose Belly Fat In FrenchPas encore d'évaluation
- Victoire totale sur toutes les maladiesD'EverandVictoire totale sur toutes les maladiesÉvaluation : 5 sur 5 étoiles5/5 (1)
- Ondes de forme vues par un physicien: Les ondes de forme ont une action bien réelleD'EverandOndes de forme vues par un physicien: Les ondes de forme ont une action bien réellePas encore d'évaluation
- Le TDAH chez l’adulte : Comment reconnaître & faire face au TDAH chez l’adulte en 30 étapes faciles.D'EverandLe TDAH chez l’adulte : Comment reconnaître & faire face au TDAH chez l’adulte en 30 étapes faciles.Pas encore d'évaluation
- Régime IG bas pour débutants : Guide pratique de la cuisine IG bas super facile avec 45 recettes IG bas pour tous les joursD'EverandRégime IG bas pour débutants : Guide pratique de la cuisine IG bas super facile avec 45 recettes IG bas pour tous les joursPas encore d'évaluation